

Efficacy of Topical Vancomycin- and Gentamicin-Loaded Calcium Sulfate Beads or Systemic Antibiotics in Eradicating Polymicrobial Biofilms Isolated from Diabetic Foot Infections within an In Vitro Wound Model
- PMID: 33753330
- PMCID: PMC8315973
- DOI: 10.1128/AAC.02012-20
Efficacy of Topical Vancomycin- and Gentamicin-Loaded Calcium Sulfate Beads or Systemic Antibiotics in Eradicating Polymicrobial Biofilms Isolated from Diabetic Foot Infections within an In Vitro Wound Model
Abstract
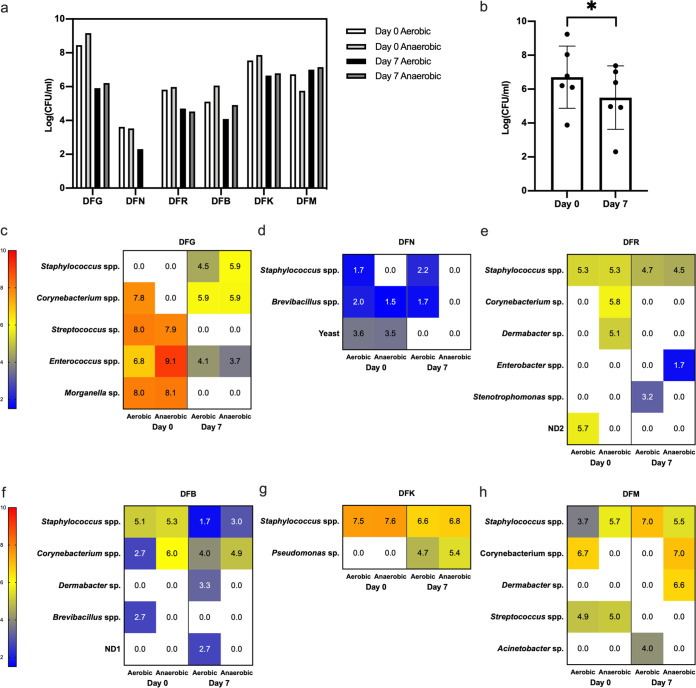
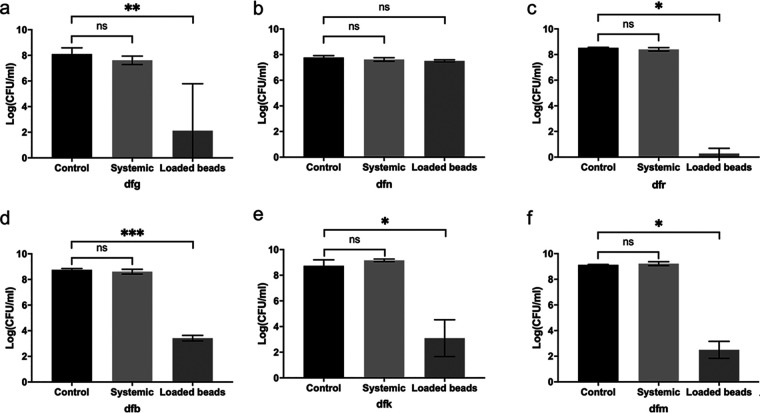
Diabetic foot ulcers are notoriously difficult to heal, with ulcers often becoming chronic, in many cases leading to amputation despite weeks or months of antibiotic therapy in addition to debridement and offloading. Alternative wound biofilm management options, such as topical rather than systemic delivery of antimicrobials, have been investigated by clinicians in order to improve treatment outcomes. Here, we collected blood and tissue from six subjects with diabetic foot infections, measured the concentrations of antibiotics in the samples after treatment, and compared the microbiota within the tissue before treatment and after 7 days of antibiotic therapy. We used an in vitro model of polymicrobial biofilm infection inoculated with isolates from the tissue we collected to simulate different methods of antibiotic administration by simulated systemic therapy or topical release from calcium sulfate beads. We saw no difference in biofilm bioburden in the models after simulated systemic therapy (representative of antibiotics used in the clinic), but we did see reductions in bioburden of between 5 and 8 logs in five of the six biofilms that we tested with topical release of antibiotics via calcium sulfate beads. Yeast is insensitive to antibiotics and was a component of the sixth biofilm. These data support further studies of the topical release of antibiotics from calcium sulfate beads in diabetic foot infections to combat the aggregate issues of infectious organisms taking the biofilm mode of growth, compromised immune involvement, and poor systemic delivery of antibiotics via the bloodstream to the site of infection in patients with diabetes.
Keywords: biofilm; clinical; diabetes; diabetic foot; infection; polymicrobial; postantibiotic effect.
Copyright © 2021 Crowther et al.
Figures
References
-
- Centre for Clinical Practice at NICE. 2011. Diabetic foot problems: inpatient management of diabetic foot problems. National Institute for Health Care Excellence, Centre for Clinical Practice at NICE, London, United Kingdom. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
