

Why women die after reaching the hospital: a qualitative critical incident analysis of the 'third delay' in postconflict northern Uganda
- PMID: 33753439
- PMCID: PMC7986759
- DOI: 10.1136/bmjopen-2020-042909
Why women die after reaching the hospital: a qualitative critical incident analysis of the 'third delay' in postconflict northern Uganda
Abstract
Objectives: To critically explore and describe the pathways that women who require emergency obstetrics and newborn care (EmONC) go through and to understand the delays in accessing EmONC after reaching a health facility in a conflict-affected setting.
Design: This was a qualitative study with two units of analysis: (1) critical incident technique (CIT) and (2) key informant interviews with health workers, patients and attendants.
Setting: Thirteen primary healthcare centres, one general private-not-for-profit hospital, one regional referral hospital and one teaching hospital in northern Uganda.
Participants: Forty-nine purposively selected health workers, patients and attendants participated in key informant interviews. CIT mapped the pathways for maternal deaths and near-misses selected based on critical case purposive sampling.
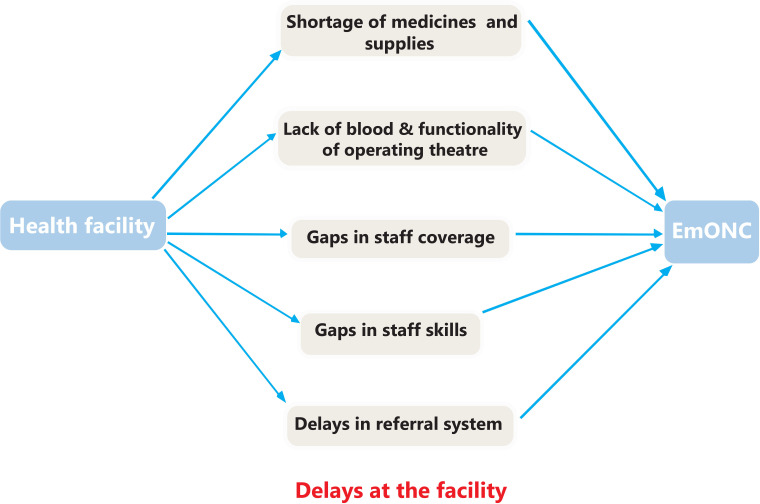
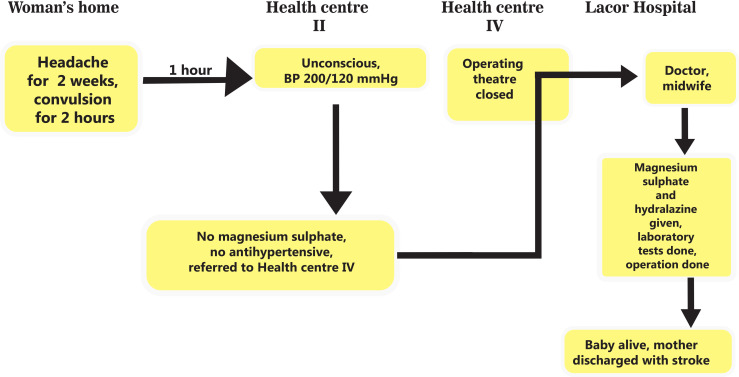
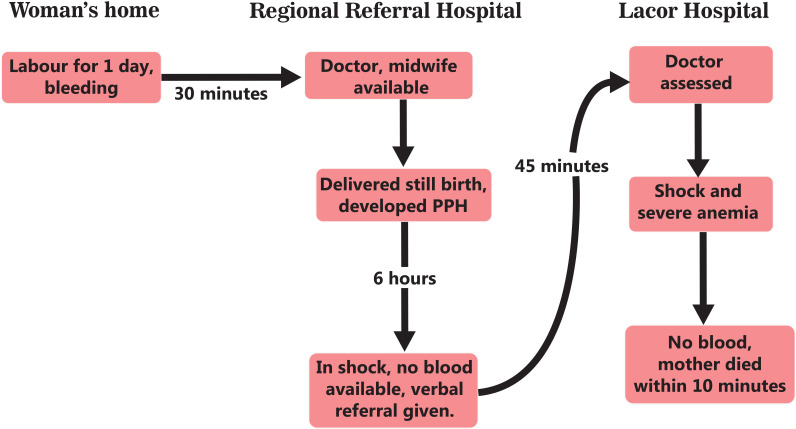
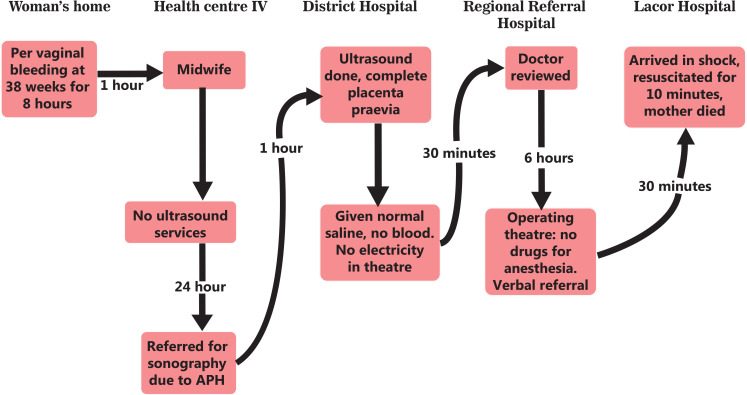
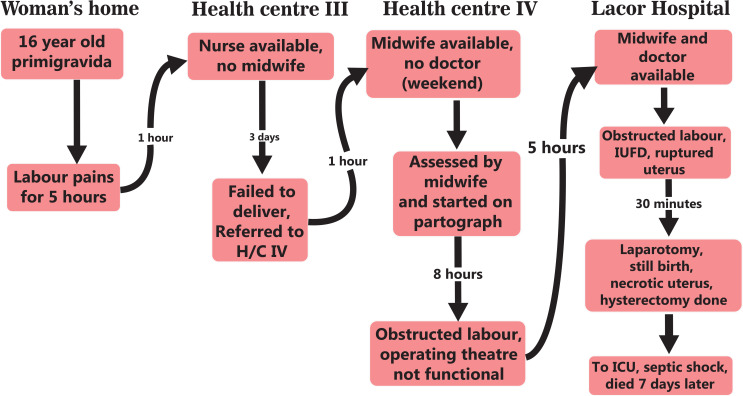
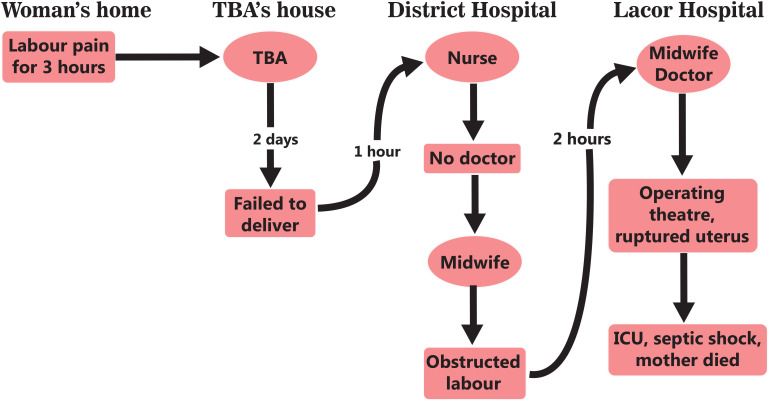
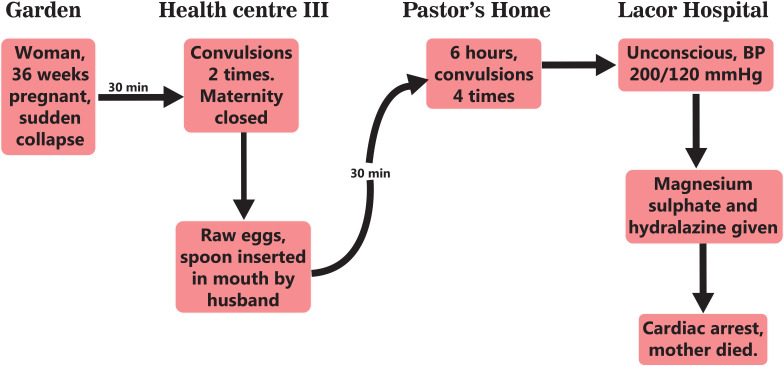
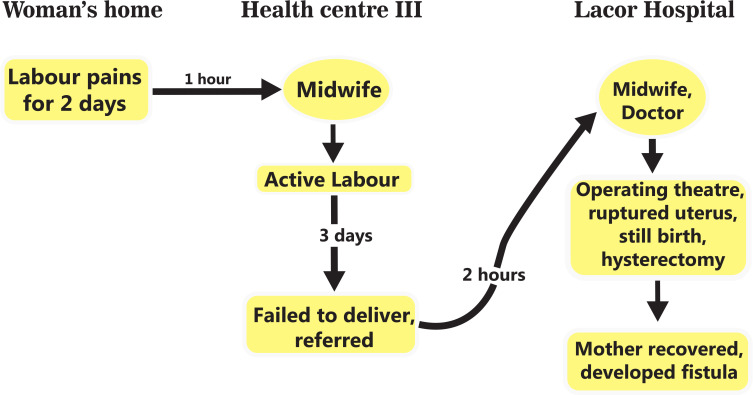
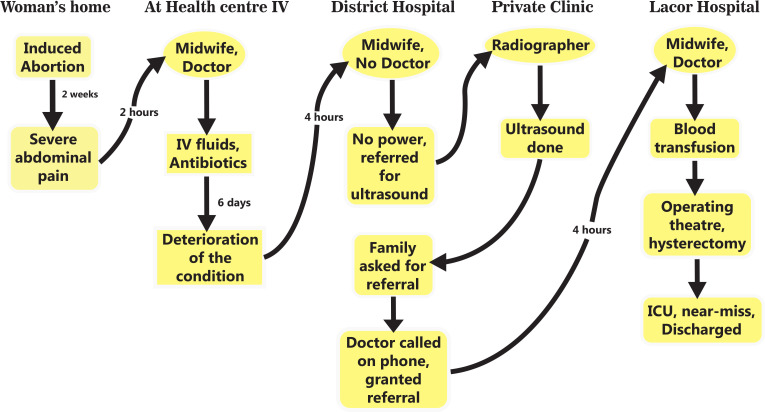
Results: After reaching the health facility, a pregnant woman goes through a complex pathway that leads to delays in receiving EmONC. Five reasons were identified for these delays: shortage of medicines and supplies, lack of blood and functionality of operating theatres, gaps in staff coverage, gaps in staff skills, and delays in the interfacility referral system. Shortage of medicines and supplies was central in most of the pathways, characterised by three patterns: delay to treat, back-and-forth movements to buy medicines or supplies, and multiple referrals across facilities. Some women also bypassed facilities they deemed to be non-functional.
Conclusion: Our findings show that the pathway to EmONC is precarious and takes too long even after making early contact with the health facility. Improvement of skills, better management of the meagre human resource and availing essential medical supplies in health facilities may help to reduce the gaps in a facility's emergency readiness and thus improve maternal and neonatal outcomes.
Keywords: gynaecology; maternal medicine; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO . Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, world bank group and the United Nations population division, 2019.
-
- Alkema L, Chou D, Hogan D, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the un maternal mortality estimation Inter-Agency group. Lancet 2016;387:462–74. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- UDHS . Uganda demographic and health survey. Kampala Uganda: Uganda Bureau of Statistics, 2011.
-
- Uganda Bureau of Statistics (UBOS) and ICF . Uganda demographic and health survey 2016: key indicators report. Rockville, Kampala, Uganda, and Maryland: UBOS, 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical