

Decision Analysis in SHared decision making for Thromboprophylaxis during Pregnancy (DASH-TOP): a sequential explanatory mixed methods pilot study protocol
- PMID: 33753445
- PMCID: PMC7986891
- DOI: 10.1136/bmjopen-2020-046021
Decision Analysis in SHared decision making for Thromboprophylaxis during Pregnancy (DASH-TOP): a sequential explanatory mixed methods pilot study protocol
Abstract
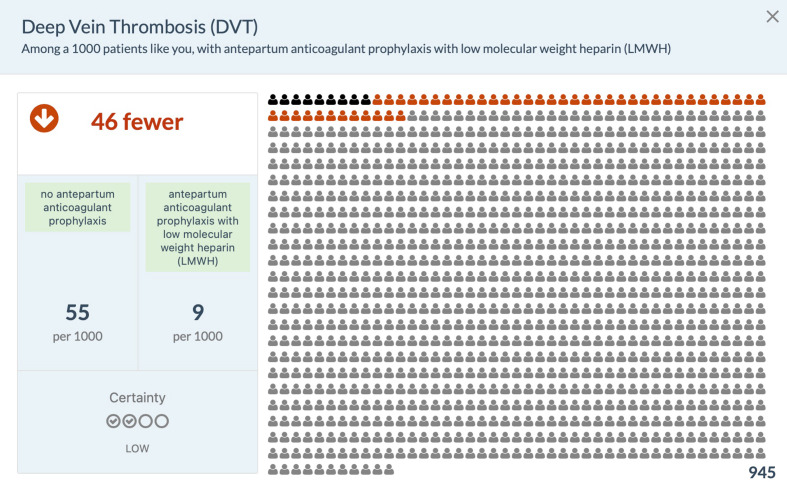
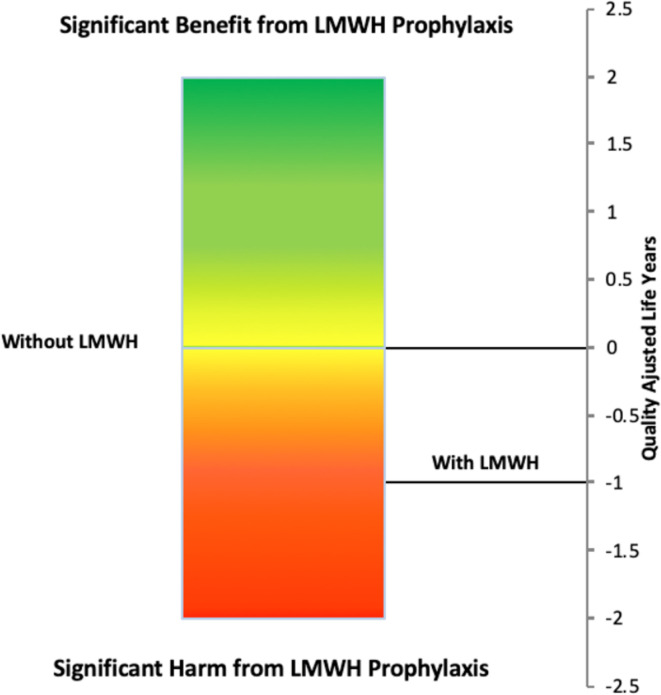
Introduction: Decision analysis is a quantitative approach to decision making that could bridge the gap between decisions based solely on evidence and the unique values and preferences of individual patients, a feature especially important when existing evidence cannot support clear recommendations and there is a close balance between harms and benefits for the treatments options under consideration. Low molecular weight heparin (LMWH) for the prevention of venous thromboembolism (VTE) during pregnancy represents one such situation. The objective of this paper is to describe the rationale and methodology of a pilot study that will explore the application of decision analysis to a shared decision-making process involving prophylactic LMWH for pregnant women or those considering pregnancy who have experienced a VTE.
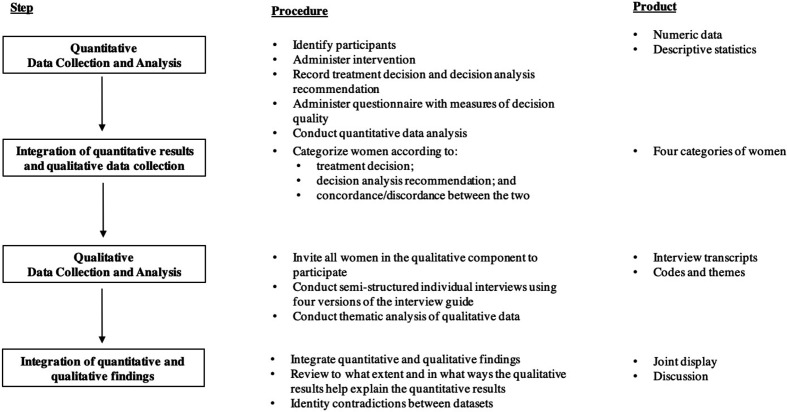
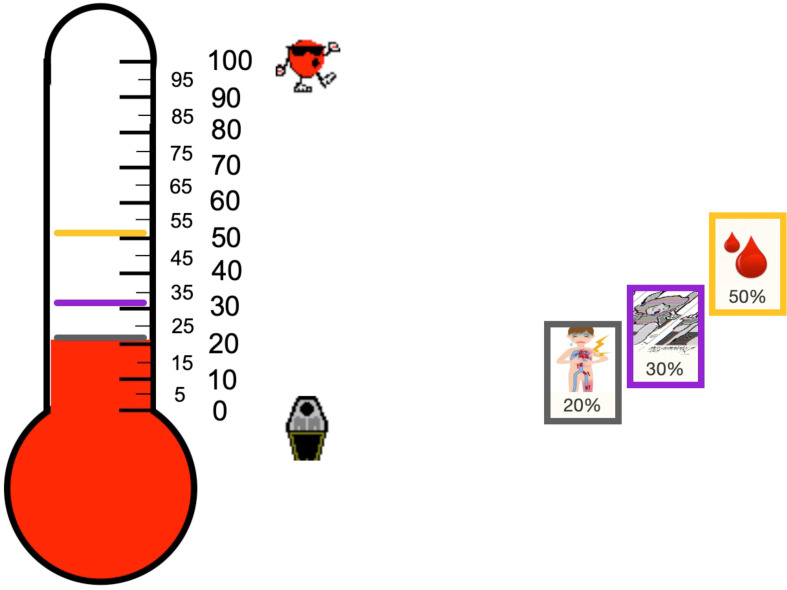
Methods and analysis: We will conduct an international, mixed methods, explanatory, sequential study, including quantitative data collection and analysis followed by qualitative data collection and analysis. In step I, we will ask women who are pregnant or considering pregnancy and have experienced VTE to participate in a shared decision-making intervention for prophylactic LMWH. The intervention consists of three components: a direct choice exercise, a values elicitation exercise and a personalised decision analysis. After administration of the intervention, we will ask women to make a treatment decision and measure decisional conflict, self-efficacy and satisfaction. In step II, which follows the analysis of quantitative data, we will use the results to inform the qualitative interview. Step III will be a qualitative descriptive study that explores participants' experiences and perceptions of the intervention. In step IV, we will integrate findings from the qualitative and quantitative analyses to obtain meta-inferences.
Ethics and dissemination: Site-specific ethics boards have approved the study. All participants will provide informed consent. The research team will take an integrated approach to knowledge translation.
Keywords: haematology; health economics; maternal medicine; thromboembolism.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ME has received grant funding from the National Institutes of Health (Eunice Kennedy Shriver National Institute of Child Health and Human Development, and National Center for Advancing Translational Sciences) and funding for investigator-initiated research from Bristol-Myers Squibb. RD has received speaking honoraria and grant funding from Ferring Inc and an early career grant from the Canadian Institutes for Health Research for projects unrelated to this study. NS has received honoraria and an educational grant from Sanofi. ML-G receives doctoral support from the Spanish Public Research Institute – Health Institute Carlos III. SB has acted as a consultant for Leo Pharma Canada (manufacturer of low molecular weight heparin) and receives unencumbered salary support through the McMaster University Eli Lilly Canada-May Cohen Chair in Women’s Health.
Figures
Similar articles
-
Assessment of a venous thromboembolism prophylaxis shared decision-making intervention (DASH-TOP) using the decisional conflict scale: a mixed-method study.BMC Med Inform Decis Mak. 2023 Nov 6;23(1):250. doi: 10.1186/s12911-023-02349-3. BMC Med Inform Decis Mak. 2023. PMID: 37932759 Free PMC article. Clinical Trial.
-
Decision Analysis in SHared decision making for Thromboprophylaxis during Pregnancy (DASH-TOP): a sequential explanatory mixed-methods pilot study.BMJ Evid Based Med. 2023 Oct;28(5):309-319. doi: 10.1136/bmjebm-2022-112098. Epub 2023 Mar 1. BMJ Evid Based Med. 2023. PMID: 36858800
-
Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition).Chest. 2008 Jun;133(6 Suppl):844S-886S. doi: 10.1378/chest.08-0761. Chest. 2008. PMID: 18574280
-
The prevention of pregnancy-related venous thromboembolism.Br J Haematol. 2015 Jan;168(2):163-74. doi: 10.1111/bjh.13159. Epub 2014 Oct 14. Br J Haematol. 2015. PMID: 25312482 Review.
-
[Thromboprophylaxis during pregnancy and the puerperium: highlights from current guidelines].Z Geburtshilfe Neonatol. 2010 Dec;214(6):217-28. doi: 10.1055/s-0030-1269861. Epub 2011 Jan 4. Z Geburtshilfe Neonatol. 2010. PMID: 21207321 Review. German.
Cited by
-
Women's values and preferences on low-molecular-weight heparin and pregnancy: a mixed-methods systematic review.BMC Pregnancy Childbirth. 2022 Oct 5;22(1):747. doi: 10.1186/s12884-022-05042-x. BMC Pregnancy Childbirth. 2022. PMID: 36199014 Free PMC article.
-
Assessment of a venous thromboembolism prophylaxis shared decision-making intervention (DASH-TOP) using the decisional conflict scale: a mixed-method study.BMC Med Inform Decis Mak. 2023 Nov 6;23(1):250. doi: 10.1186/s12911-023-02349-3. BMC Med Inform Decis Mak. 2023. PMID: 37932759 Free PMC article. Clinical Trial.
References
-
- Knight M, Nair M, Tuffnell D, . Saving Lives, Improving Mothers’ Care - Lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2013–15. Oxford: National Perinatal Epidemiology Unit, University of Oxford, 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous