

Molecular imaging and biochemical response assessment after a single cycle of [225Ac]Ac-PSMA-617/[177Lu]Lu-PSMA-617 tandem therapy in mCRPC patients who have progressed on [177Lu]Lu-PSMA-617 monotherapy
- PMID: 33754047
- PMCID: PMC7977444
- DOI: 10.7150/thno.56211
Molecular imaging and biochemical response assessment after a single cycle of [225Ac]Ac-PSMA-617/[177Lu]Lu-PSMA-617 tandem therapy in mCRPC patients who have progressed on [177Lu]Lu-PSMA-617 monotherapy
Abstract
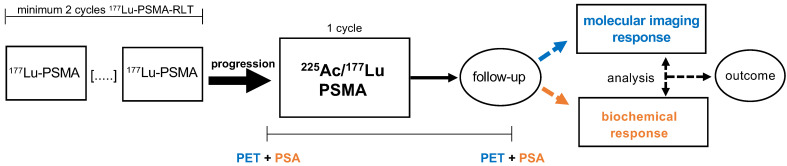
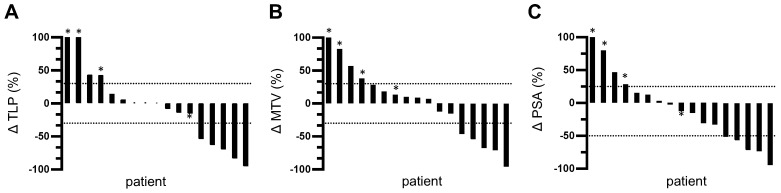
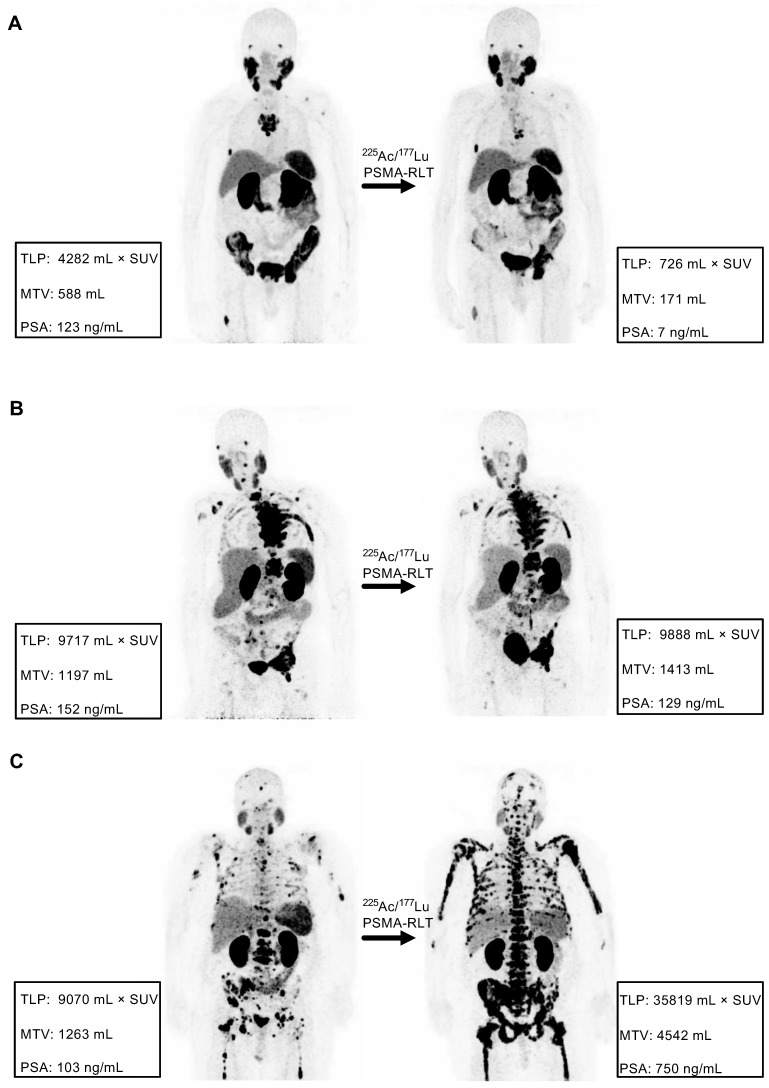
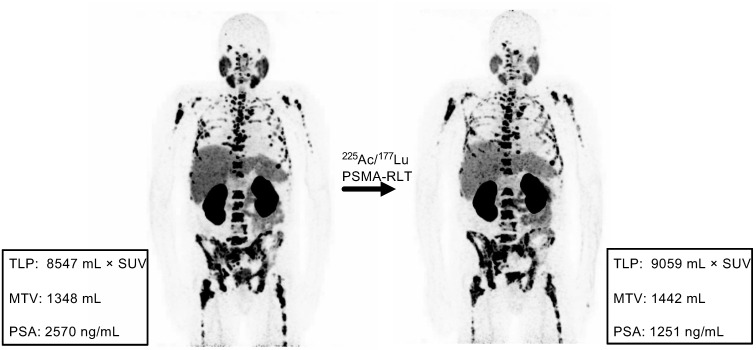
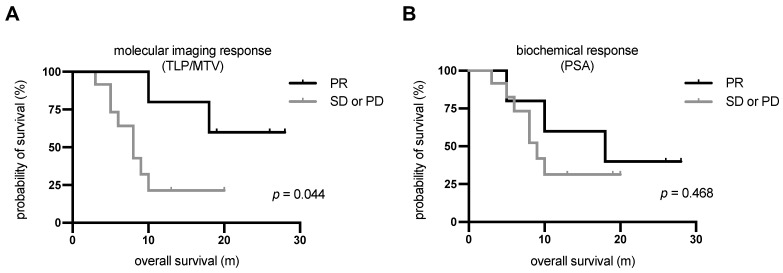
Rationale: Despite the promising results of prostate-specific membrane antigen (PSMA)-targeted 177Lu radioligand therapy in metastatic castration-resistant prostate carcinoma (mCRPC), some patients do not respond and other patients with initially good response develop resistance to this treatment. In this study, we investigated molecular imaging and biochemical responses after a single cycle of [225Ac]Ac-PSMA-617/[177Lu]Lu-PSMA-617 tandem therapy in patients who had progressed on [177Lu]Lu-PSMA-617 monotherapy. Methods: Seventeen patients with mCRPC were included in a retrospective, monocenter study. Molecular imaging-based response was assessed by modified PERCIST criteria using the whole-body total lesion PSMA (TLP) and molecular tumour volume (MTV) derived from [68Ga]Ga-PSMA-11 PET/CT. Biochemical response was evaluated according to PCWG3 criteria using the prostate-specific antigen (PSA) serum value. Concordance and correlation statistics as well as survival analyses were performed. Results: Based on the molecular imaging-based response assessment, 5 (29.4%) patients showed partial remission and 7 (41.2%) had stable disease. The remaining 5 (29.4%) patients had further progression, four with an increase in TLP/MTV of >30% and one with stable TLP/MTV but appearance of new metastases. Based on the biochemical response assessment, 5 (29.4%), 8 (47.1%), and 4 (23.5%) patients showed partial remission, stable disease, and progressive disease, respectively. A comparison of the response assessment methods showed a concordance of 100% (17/17) between TLP and MTV and 70.6% (12/17) between TLP/MTV and PSA. Patients with partial remission, independently assessed by each method, had better overall survival (OS) than patients with either stable or progressive disease. The difference in OS was statistically significant for the molecular imaging response assessment (median OS not reached vs. 8.3 m, p = 0.044), but not for the biochemical response assessment (median OS 18.1 m vs. 9.4 m, p = 0.468). Conclusion: Based on both assessment methods, [225Ac]Ac-PSMA-617/[177Lu]Lu-PSMA-617 tandem therapy is an effective treatment for the highly challenging cohort of patients with mCRPC who have progressed on [177Lu]Lu-PSMA-617 monotherapy. Molecular imaging response and biochemical PSA response were mostly concordant, though a considerable number of cases (29.4%) were discordant. Molecular imaging response reflecting the change in total viable tumour burden appears to be superior to PSA change in estimating survival outcome after tandem therapy.
Keywords: 225Ac and 177Lu; Biochemical response; Metastatic castration-resistant prostate cancer.; Molecular imaging response; PSMA radioligand therapy.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Kirby M, Hirst C, Crawford ED. Characterising the castration-resistant prostate cancer population: a systematic review: The Epidemiology of CRPC. Int J Clin Pract. 2011;65:1180–92. - PubMed
-
- Tannock IF, Horti J, Oudard S, James ND, Rosenthal MA. Docetaxel plus Prednisone or Mitoxantrone plus Prednisone for Advanced Prostate Cancer. N Engl J Med. 2004;351:1502–12. - PubMed
-
- Berthold DR, Pond GR, Soban F, de Wit R, Eisenberger M, Tannock IF. Docetaxel Plus Prednisone or Mitoxantrone Plus Prednisone for Advanced Prostate Cancer: Updated Survival in the TAX 327 Study. J Clin Oncol. 2008;26:242–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
