

Laboratory, Clinical, and Survival Outcomes Associated With Peptide Receptor Radionuclide Therapy in Patients With Gastroenteropancreatic Neuroendocrine Tumors
- PMID: 33755166
- PMCID: PMC7988364
- DOI: 10.1001/jamanetworkopen.2021.2274
Laboratory, Clinical, and Survival Outcomes Associated With Peptide Receptor Radionuclide Therapy in Patients With Gastroenteropancreatic Neuroendocrine Tumors
Abstract
Importance: Peptide receptor radionuclide therapy (PRRT) is approved in the US for treatment of gastroenteropancreatic neuroendocrine tumors (NETs), but data on PRRT outcomes within US populations remain scarce.
Objective: To analyze the first 2 years of PRRT implementation at a US-based NET referral center.
Design, setting, and participants: This cohort study was conducted using medical records of patients with metastatic NET receiving PRRT from 2018 through 2020 in a NET program at a tertiary referral center. Included patients were those at the center with metastatic NETs who received at least 1 dose of PRRT over the study period. Laboratory toxic effects were assessed using Common Terminology Criteria for Adverse Events version 5.0. Tumor response was determined using Response Evaluation Criteria in Solid Tumors 1.1. Survival analysis was conducted to identify factors associated with progression-free survival (PFS) and overall survival. Data were analyzed from August 2018 through August 2020.
Exposures: Receiving 4 cycles of lutetium-177-dotatate infusion, separated by 8-week intervals targeted to 7.4 GBq (200 mCi) per dose.
Main outcomes and measures: Data were compared from before and after PRRT to determine hematologic, liver, and kidney toxic effects and to assess tumor progression and patient survival.
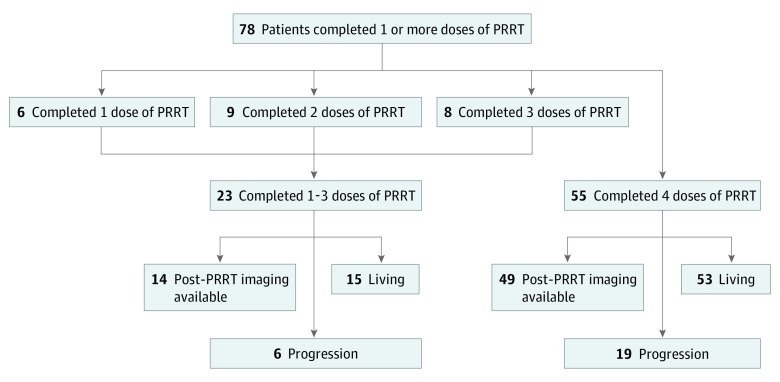
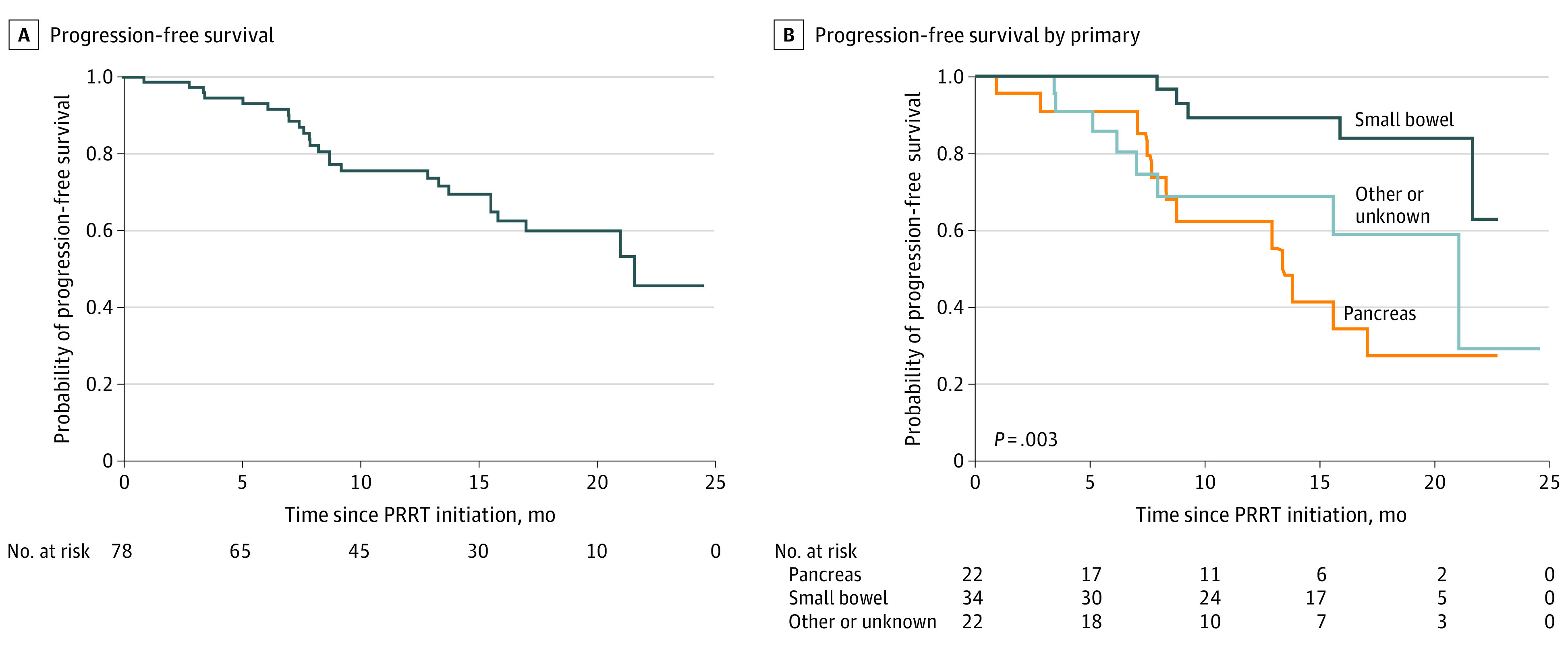
Results: Among 78 patients receiving at least 1 dose of PRRT, median (interquartile range) age at PRRT initiation was 59.8 (53.5-69.2) years and 39 (50.0%) were men. The most common primary NET sites included small bowel, occurring in 34 patients (43.6%), and pancreas, occurring in 22 patients (28.2%). World Health Organization grade 1 or 2 tumors occurred in 62 patients (79.5%). Among all patients, 56 patients underwent pretreatment with tumor resection (71.8%), 49 patients received nonsomatostatin analogue systemic therapy (62.8%), and 49 patients received liver-directed therapy (62.8%). At least 1 grade 2 or greater toxic effect was found in 47 patients (60.3%). Median PFS was 21.6 months for the study group, was not reached by 22 months for patients with small bowel primary tumors, and was 13.3 months for patients with pancreatic primary tumors. Having a small bowel primary tumor was associated with a lower rate of progression compared with having a pancreatic primary tumor (hazard ratio, 0.19; 95% CI, 0.07-0.55; P = .01). Median overall survival was not reached.
Conclusions and relevance: This cohort study of patients with metastatic NETs found that PRRT was associated with laboratory-measured toxic effects during treatment for most patients and an overall median PFS of 21.6 months. Patients with small bowel NETs had longer PFS after PRRT compared with patients with pancreatic NETs.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
