

Patterns and persistence of SARS-CoV-2 IgG antibodies in Chicago to monitor COVID-19 exposure
- PMID: 33755598
- PMCID: PMC8262291
- DOI: 10.1172/jci.insight.146148
Patterns and persistence of SARS-CoV-2 IgG antibodies in Chicago to monitor COVID-19 exposure
Abstract
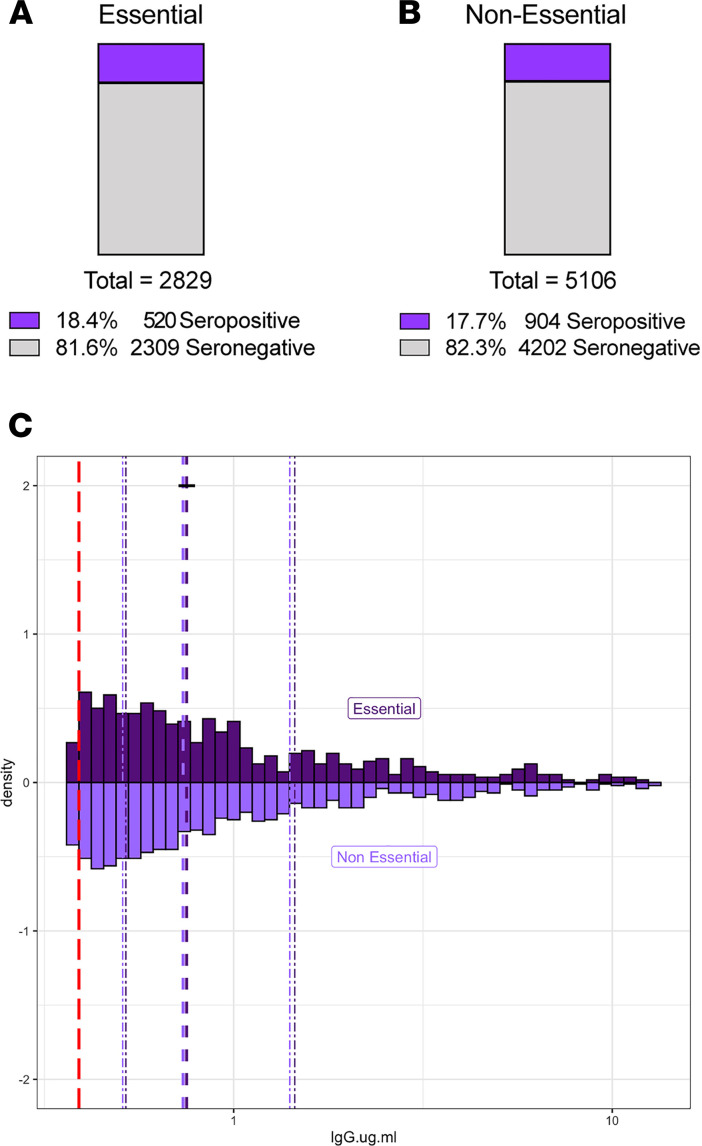
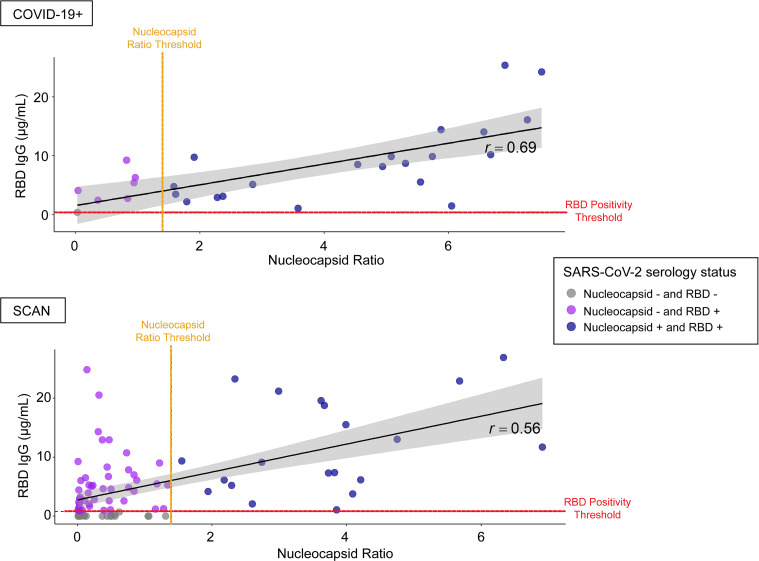
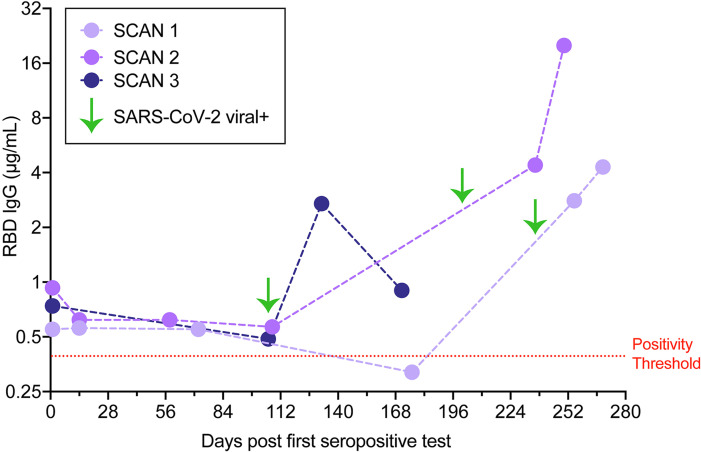
BACKGROUNDEstimates of seroprevalence to SARS-CoV-2 vary widely and may influence vaccination response. We ascertained IgG levels across a single US metropolitan site, Chicago, from June 2020 through December 2020.METHODSParticipants (n = 7935) were recruited through electronic advertising and received materials for a self-sampled dried-blood spot assay through the mail or a minimal contact in-person method. IgG against the receptor-binding domain of SARS-CoV-2 was measured using an established highly sensitive and highly specific assay.RESULTSOverall seroprevalence was 17.9%, with no significant difference between method of contact. Only 2.5% of participants reported having had a diagnosis of COVID-19 based on virus detection, consistent with a 7-fold greater exposure to SARS-CoV-2 measured by serology than that detected by viral testing. The range of IgG level observed in seropositive participants from this community survey overlapped with the range of IgG levels associated with COVID-19 cases having a documented positive PCR test. From a subset of those who participated in repeat testing, half of seropositive individuals retained detectable antibodies for 3 to 4 months.CONCLUSIONQuantitative IgG measurements with a highly specific and sensitive assay indicated more widespread exposure to SARS-CoV-2 than observed by viral testing. The range of IgG concentrations produced from these asymptomatic exposures was similar to IgG levels occurring after documented nonhospitalized COVID-19, which were considerably lower than those produced from hospitalized COVID-19 cases. The differing ranges of IgG response, coupled with the rate of decay of antibodies, may influence response to subsequent viral exposure and vaccine.FundingNational Science Foundation grant 2035114, NIH grant 3UL1TR001422-06S4, NIH National Center for Advancing Translational Sciences grants UL1 TR001422 and UL1 TR002389, Dixon Family Foundation, Northwestern University Cancer Center (NIH grant P30 CA060553), and Walder Foundation's Chicago Coronavirus Assessment Network.
Keywords: COVID-19; Immunoglobulins.
Conflict of interest statement
Figures



Update of
-
Patterns and persistence of SARS-CoV-2 IgG antibodies in Chicago to monitor COVID-19 exposure.medRxiv [Preprint]. 2021 Mar 16:2020.11.17.20233452. doi: 10.1101/2020.11.17.20233452. medRxiv. 2021. Update in: JCI Insight. 2021 May 10;6(9):146148. doi: 10.1172/jci.insight.146148. PMID: 33236031 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
