

Carotid plaque inflammatory activity assessed by 2-[18F]FDG-PET imaging decrease after a neurological thromboembolic event
- PMID: 33755791
- PMCID: PMC7988031
- DOI: 10.1186/s13550-021-00773-y
Carotid plaque inflammatory activity assessed by 2-[18F]FDG-PET imaging decrease after a neurological thromboembolic event
Abstract
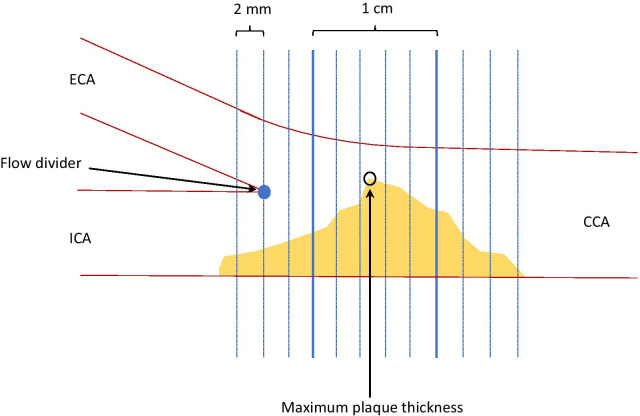
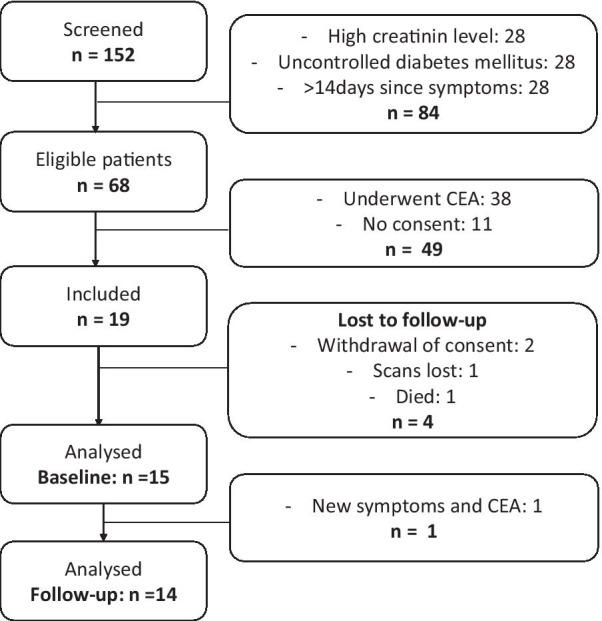
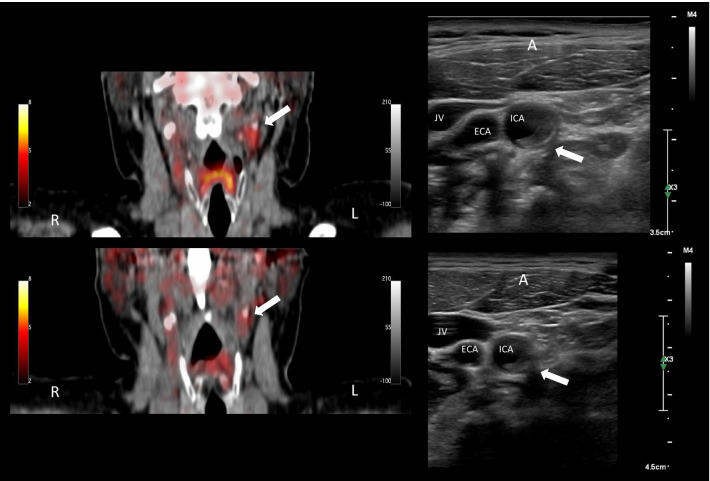
Background: Atherosclerotic plaque vulnerability is comprised by plaque composition driven by inflammatory activity and these features can be depicted with 3D ultrasound and 2-[18F]FDG-PET, respectively. The study investigated timely changes in carotid artery plaque inflammation and morphology after a thromboembolic event with PET/CT and novel ultrasound volumetric grayscale median (GSM) readings. Patients with a single hemisphere-specific neurological symptom and the presence of an ipsilateral carotid artery atherosclerotic plaque were prospectively included to both 2-[18F]FDG PET/CT and 3D ultrasound scans of the plaque immediately after their event and again three months later. On PET/CT images the maximum standardized uptake value (SUVmax) was measured and the volumetric ultrasound acquisitions were analyzed using a semiautomated software measuring GSM values.
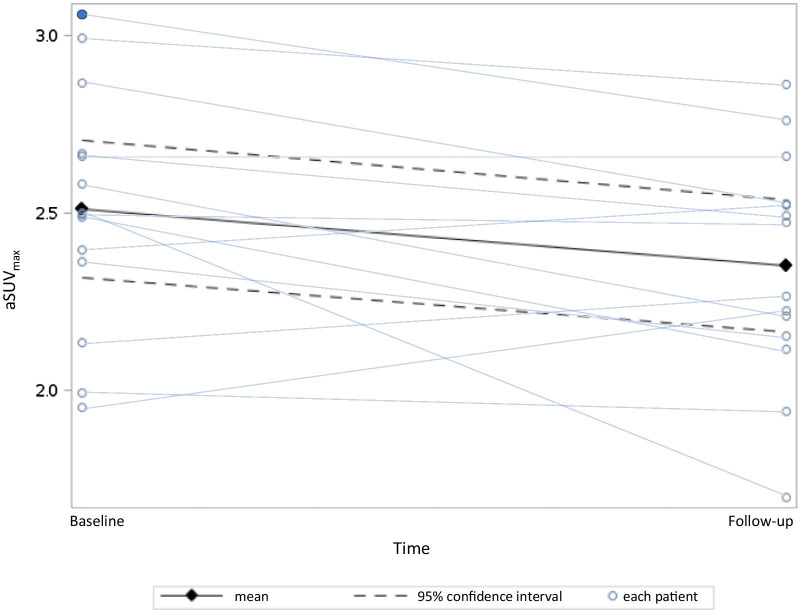
Results: Baseline scans were performed by a mean of 7 days (range 2-14) after the symptom and again after 98 days (range 91-176). For the entire group (n = 14), we found a decrease in average SUVmax from baseline to follow-up of - 0.18 (95% confidence interval: - 0.34 to - 0.02, P = 0.034). GSM did not increase significantly over time (mean change: + 2.21, 95% confidence interval: - 17.02 to 21.44, P = 0.808).
Conclusion: A decrease in culprit lesion 2-[18F]FDG-uptake 3 months after an event indicates a decrease in inflammatory activity, suggesting that carotid plaque stabilization over time. 3D ultrasound morphological quantitative differences in GSM were not detectable after 3 months.
Keywords: 3D ultrasound; Carotid artery plaque; FDG PET; Inflammation; Vulnerable plaque.
Conflict of interest statement
Henrik Sillesen has received research grants and speakers honoraria from Philips Ultrasound.
Figures
References
-
- Naylor AR, Ricco JB, de Borst GJ, Debus S, de Haro J, Halliday A, et al. Editor's choice—management of atherosclerotic carotid and vertebral artery disease: 2017 clinical practice guidelines of the European Society for Vascular Surgery (ESVS) Eur J Vasc Endovasc Surg. 2018;55(1):3–81. doi: 10.1016/j.ejvs.2017.06.021. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
