

SARS-CoV-2-specific serological and functional T cell immune responses during acute and early COVID-19 convalescence in solid organ transplant patients
- PMID: 33756051
- PMCID: PMC8251492
- DOI: 10.1111/ajt.16570
SARS-CoV-2-specific serological and functional T cell immune responses during acute and early COVID-19 convalescence in solid organ transplant patients
Abstract
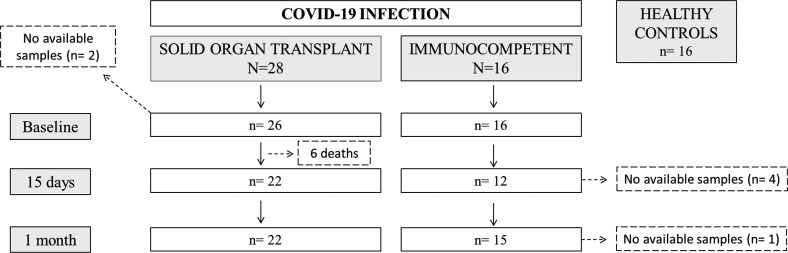
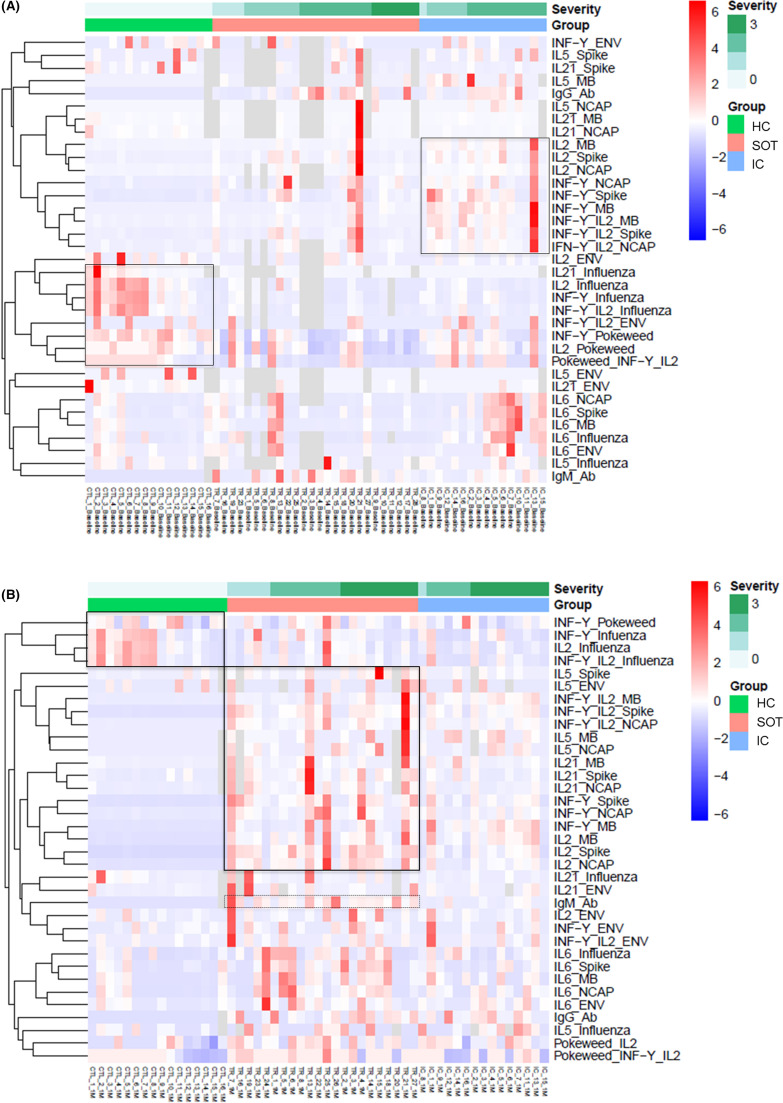
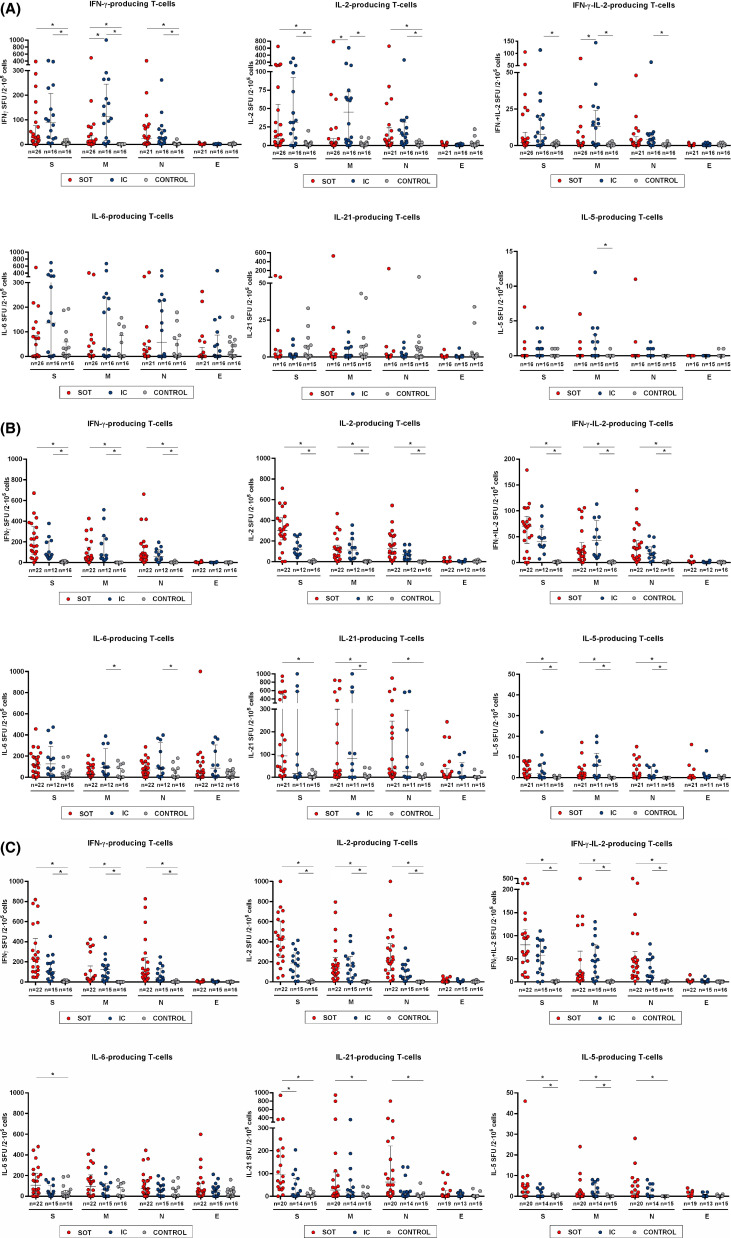
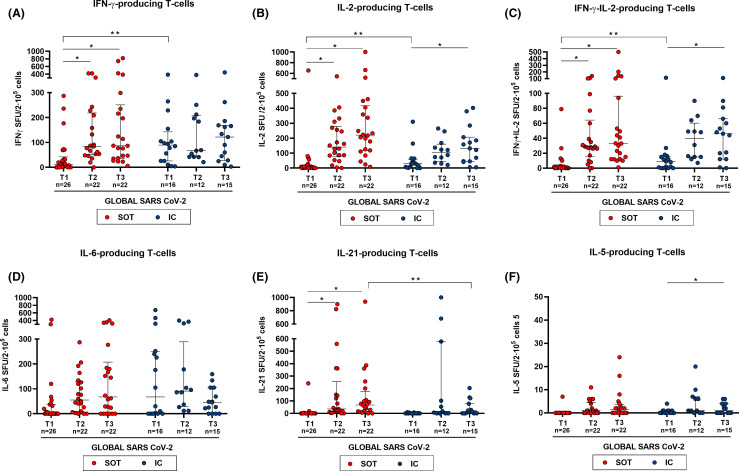
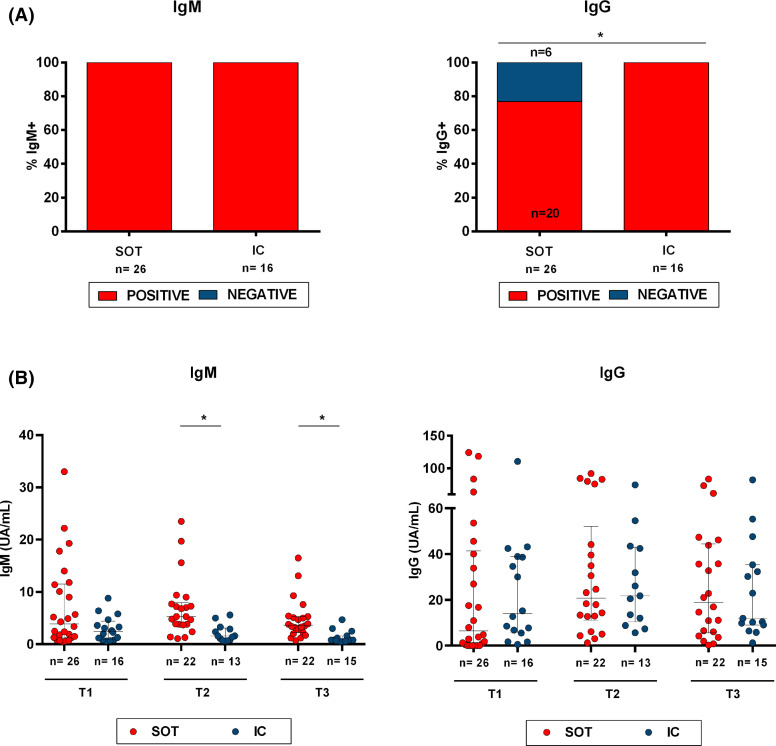
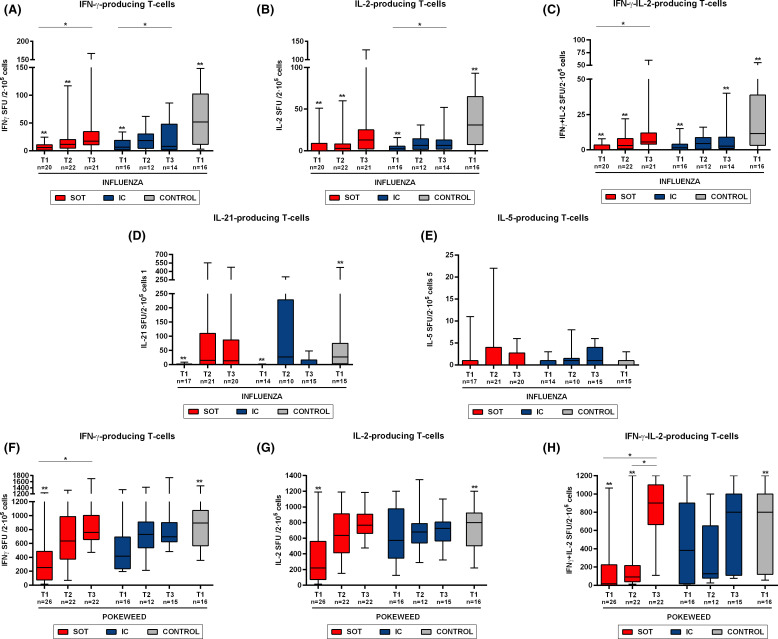
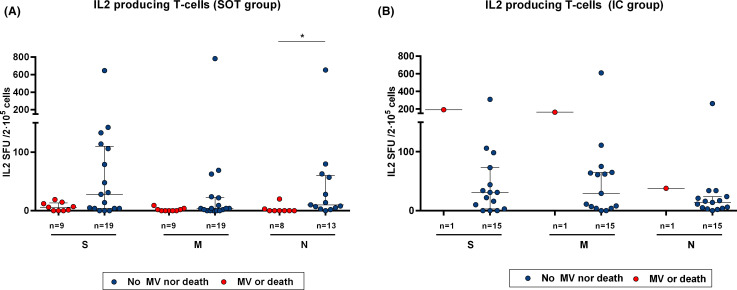
The description of protective humoral and T cell immune responses specific against SARS-CoV-2 has been reported among immunocompetent (IC) individuals developing COVID-19 infection. However, its characterization and determinants of poorer outcomes among the at-risk solid organ transplant (SOT) patient population have not been thoroughly investigated. Cytokine-producing T cell responses, such as IFN-γ, IL-2, IFN-γ/IL-2, IL-6, IL-21, and IL-5, against main immunogenic SARS-CoV-2 antigens and IgM/IgG serological immunity were tracked in SOT (n = 28) during acute infection and at two consecutive time points over the following 40 days of convalescence and were compared to matched IC (n = 16) patients admitted with similar moderate/severe COVID-19. We describe the development of a robust serological and functional T cell immune responses against SARS-CoV-2 among SOT patients, similar to IC patients during early convalescence. However, at the infection onset, SOT displayed lower IgG seroconversion rates (77% vs. 100%; p = .044), despite no differences on IgG titers, and a trend toward decreased SARS-CoV-2-reactive T cell frequencies, especially against the membrane protein (7 [0-34] vs. 113 [15-245], p = .011, 2 [0-9] vs. 45 [5-74], p = .009, and 0 [0-2] vs. 13 [1-24], p = .020, IFN-γ, IL-2, and IFN-γ/IL-2 spots, respectively). In summary, our data suggest that despite a certain initial delay, SOT population achieve comparable functional immune responses than the general population after moderate/severe COVID-19.
Keywords: COVID-19 infection; T cell biology; adaptive immunity; basic (laboratory) research / science; clinical research / practice; heart transplantation / cardiology; infection and infectious agents; kidney transplantation / nephrology; liver transplantation / hepatology; solid organ transplantation.
© 2021 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the chinese center for disease control and prevention. JAMA - J Am Med Assoc. 2020;323(13):1239–1242. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
