

Integrating No.3 lymph nodes and primary tumor radiomics to predict lymph node metastasis in T1-2 gastric cancer
- PMID: 33757460
- PMCID: PMC7989204
- DOI: 10.1186/s12880-021-00587-3
Integrating No.3 lymph nodes and primary tumor radiomics to predict lymph node metastasis in T1-2 gastric cancer
Abstract
Background: This study aimed to develope and validate a radiomics nomogram by integrating the quantitative radiomics characteristics of No.3 lymph nodes (LNs) and primary tumors to better predict preoperative lymph node metastasis (LNM) in T1-2 gastric cancer (GC) patients.
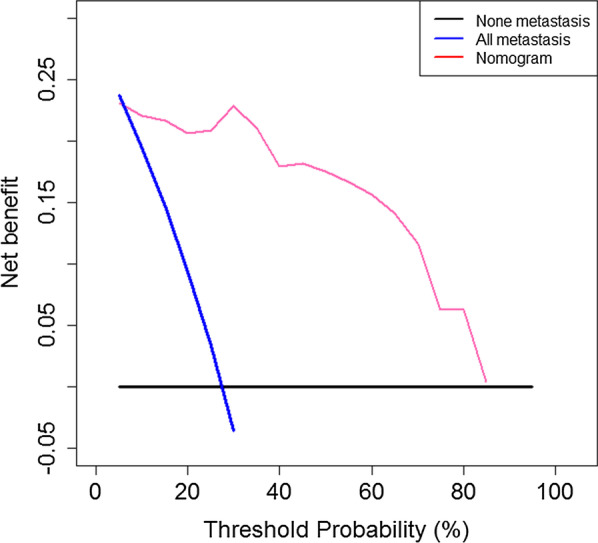
Methods: A total of 159 T1-2 GC patients who had undergone surgery with lymphadenectomy between March 2012 and November 2017 were retrospectively collected and divided into a training cohort (n = 80) and a testing cohort (n = 79). Radiomic features were extracted from both tumor region and No. 3 station LNs based on computed tomography (CT) images per patient. Then, key features were selected using minimum redundancy maximum relevance algorithm and fed into two radiomic signatures, respectively. Meanwhile, the predictive performance of clinical risk factors was studied. Finally, a nomogram was built by merging radiomic signatures and clinical risk factors and evaluated by the area under the receiver operator characteristic curve (AUC) as well as decision curve.
Results: Two radiomic signatures, reflecting phenotypes of the tumor and LNs respectively, were significantly associated with LN metastasis. A nomogram incorporating two radiomic signatures and CT-reported LN metastasis status showed good discrimination of LN metastasis in both the training cohort (AUC 0.915; 95% confidence interval [CI] 0.832-0.998) and testing cohort (AUC 0.908; 95% CI 0.814-1.000). The decision curve also indicated its potential clinical usefulness.
Conclusions: The nomogram received favorable predictive accuracy in predicting No.3 LNM in T1-2 GC, and the nomogram showed positive role in predicting LNM in No.4 LNs. The nomogram may be used to predict LNM in T1-2 GC and could assist the choice of therapy.
Keywords: Lymph nodes; Nomogram; Stomach cancer.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
CT-based radiomics nomogram for preoperative prediction of No.10 lymph nodes metastasis in advanced proximal gastric cancer.Eur J Surg Oncol. 2021 Jun;47(6):1458-1465. doi: 10.1016/j.ejso.2020.11.132. Epub 2020 Nov 24. Eur J Surg Oncol. 2021. PMID: 33261951
-
CT radiomics nomogram for the preoperative prediction of lymph node metastasis in gastric cancer.Eur Radiol. 2020 Feb;30(2):976-986. doi: 10.1007/s00330-019-06398-z. Epub 2019 Aug 29. Eur Radiol. 2020. PMID: 31468157
-
A Comprehensive Nomogram Combining CT Imaging with Clinical Features for Prediction of Lymph Node Metastasis in Stage I-IIIB Non-small Cell Lung Cancer.Ther Innov Regul Sci. 2022 Jan;56(1):155-167. doi: 10.1007/s43441-021-00345-1. Epub 2021 Oct 26. Ther Innov Regul Sci. 2022. PMID: 34699046
-
Predictive value of radiomic features extracted from primary lung adenocarcinoma in forecasting thoracic lymph node metastasis: a systematic review and meta-analysis.BMC Pulm Med. 2024 May 18;24(1):246. doi: 10.1186/s12890-024-03020-x. BMC Pulm Med. 2024. PMID: 38762472 Free PMC article.
-
Diagnostic accuracy of CT-based radiomics and deep learning for predicting lymph node metastasis in esophageal cancer.Clin Imaging. 2024 Sep;113:110225. doi: 10.1016/j.clinimag.2024.110225. Epub 2024 Jun 16. Clin Imaging. 2024. PMID: 38905878
Cited by
-
Applications of Artificial Intelligence for Metastatic Gastrointestinal Cancer: A Systematic Literature Review.Cancers (Basel). 2025 Feb 6;17(3):558. doi: 10.3390/cancers17030558. Cancers (Basel). 2025. PMID: 39941923 Free PMC article. Review.
-
Preoperative predictive model for the probability of lymph node metastasis in gastric cancer: a retrospective study.Front Oncol. 2024 Sep 27;14:1473423. doi: 10.3389/fonc.2024.1473423. eCollection 2024. Front Oncol. 2024. PMID: 39399177 Free PMC article.
-
Diagnostic performance of CT scan-based radiomics for prediction of lymph node metastasis in gastric cancer: a systematic review and meta-analysis.Front Oncol. 2023 Oct 23;13:1185663. doi: 10.3389/fonc.2023.1185663. eCollection 2023. Front Oncol. 2023. PMID: 37936604 Free PMC article.
-
Role of radiomics in the diagnosis and treatment of gastrointestinal cancer.World J Gastroenterol. 2022 Nov 14;28(42):6002-6016. doi: 10.3748/wjg.v28.i42.6002. World J Gastroenterol. 2022. PMID: 36405385 Free PMC article. Review.
-
Role of radiomics in predicting lymph node metastasis in gastric cancer: a systematic review.Front Med (Lausanne). 2023 Aug 16;10:1189740. doi: 10.3389/fmed.2023.1189740. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37663653 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
