

Electrocardiographic manifestations in a large right-sided pneumothorax
- PMID: 33757495
- PMCID: PMC7989373
- DOI: 10.1186/s12890-021-01470-1
Electrocardiographic manifestations in a large right-sided pneumothorax
Abstract
Background: Pneumothorax is an extrapulmonary air accumulation within the pleural space between the lung and chest wall. Once pneumothorax acquires tension physiology, it turns into a potentially lethal condition requiring prompt surgical intervention. Common symptoms are chest pain and dyspnea; hence an electrocardiogram (ECG) is often performed in emergent settings. However, early diagnosis of pneumothorax remains challenging since chest pain and dyspnea are common symptomatology in various life-threatening emergencies, often leading to overlooked or delayed diagnosis. While the majority of left-sided pneumothorax-related ECG abnormalities have been reported, right-sided pneumothorax-related ECG abnormalities remain elucidated.
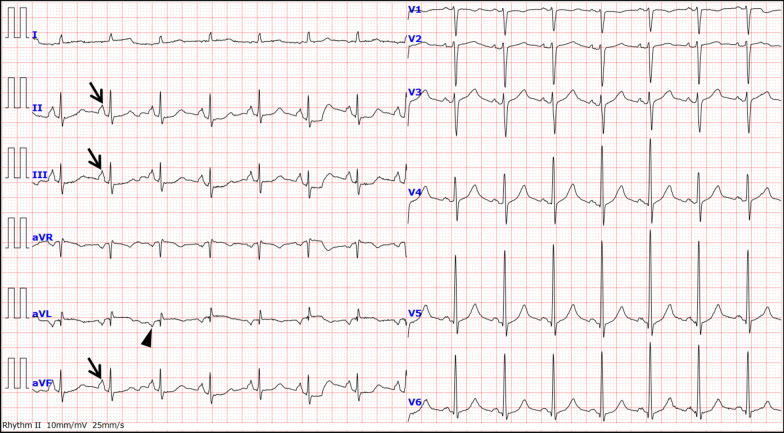
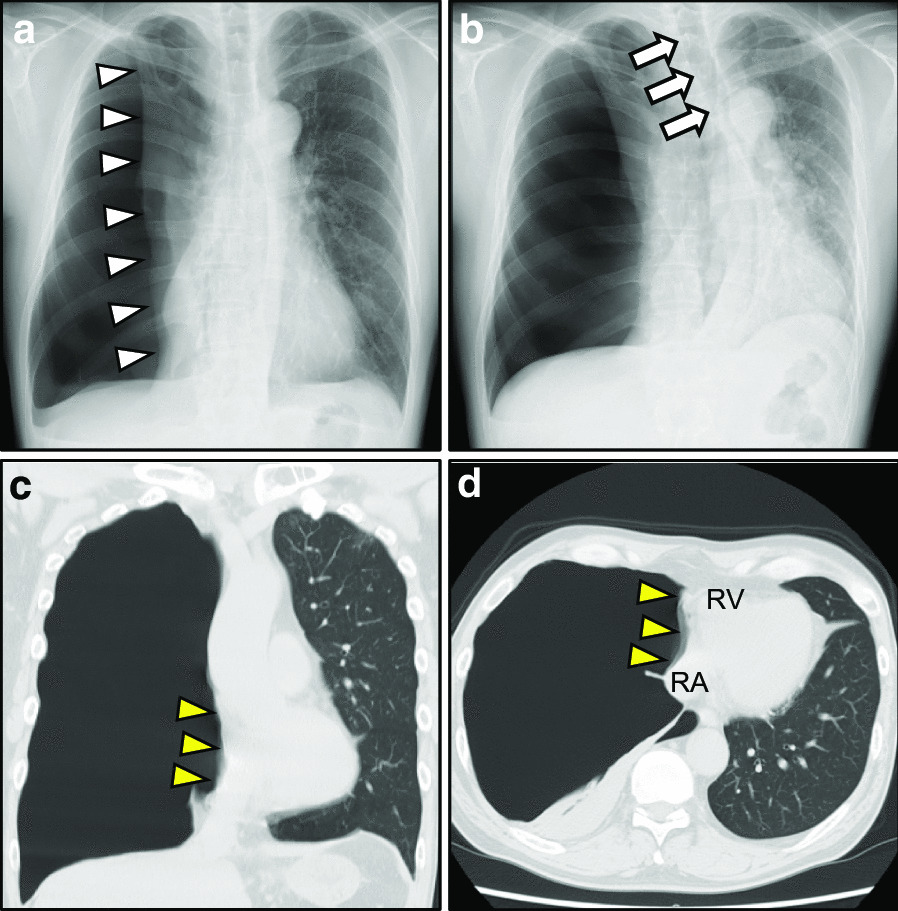
Case presentation: A 51-year-old man presented to the emergency department with acute-onset chest pain and dyspnea. Upon initial examination, the patient had a blood pressure of 98/68 mmHg, tachycardia of 100 beats/min, tachypnea of 28 breaths/min, and oxygen saturation of 94% on ambient air. Chest auscultation revealed decreased breath sounds on the right side. ECG revealed sinus tachycardia, phasic voltage variation of QRS complexes in V4-6, P-pulmonale, and vertical P-wave axis. Chest radiographs and computed tomography (CT) scans confirmed a large right-sided pneumothorax. The patient's symptoms, all the ECG abnormalities, and increased heart rate on the initial presentation resolved following an emergent tube thoracostomy. Moreover, we found that these ECG abnormalities consisted of two independent factors: respiratory components and the diaphragm level. Besides, CT scans demonstrated the large bullae with a maximum diameter of 46 × 49 mm in the right lung apex. Finally, the patient showed complete recovery with a thoracoscopic bullectomy.
Conclusions: Herein, we describe a case of a large right-sided primary spontaneous pneumothorax with characteristic ECG findings that resolved following re-expansion of the lung. Our case may shed new light on the mechanisms underlying ECG abnormalities associated with a large right-sided pneumothorax. Moreover, ECG manifestations may provide useful information to suspect a large pneumothorax or tension pneumothorax in emergent settings where ECGs are performed on patients with acute chest pain and dyspnea.
Keywords: Chest pain; Electrocardiogram; P-pulmonale; Phasic voltage variation; Right-sided pneumothorax; Vertical P-wave axis.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Krenke R, Nasilowski J, Przybylowski T, Chazan R. Electrocardiographic changes in patients with spontaneous pneumothorax. J Physiol Pharmacol. 2008;59(Suppl 6):361–373. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
