

Percutaneous nephrostomy versus retrograde ureteral stenting for acute upper obstructive uropathy: a systematic review and meta-analysis
- PMID: 33758312
- PMCID: PMC7988020
- DOI: 10.1038/s41598-021-86136-y
Percutaneous nephrostomy versus retrograde ureteral stenting for acute upper obstructive uropathy: a systematic review and meta-analysis
Abstract
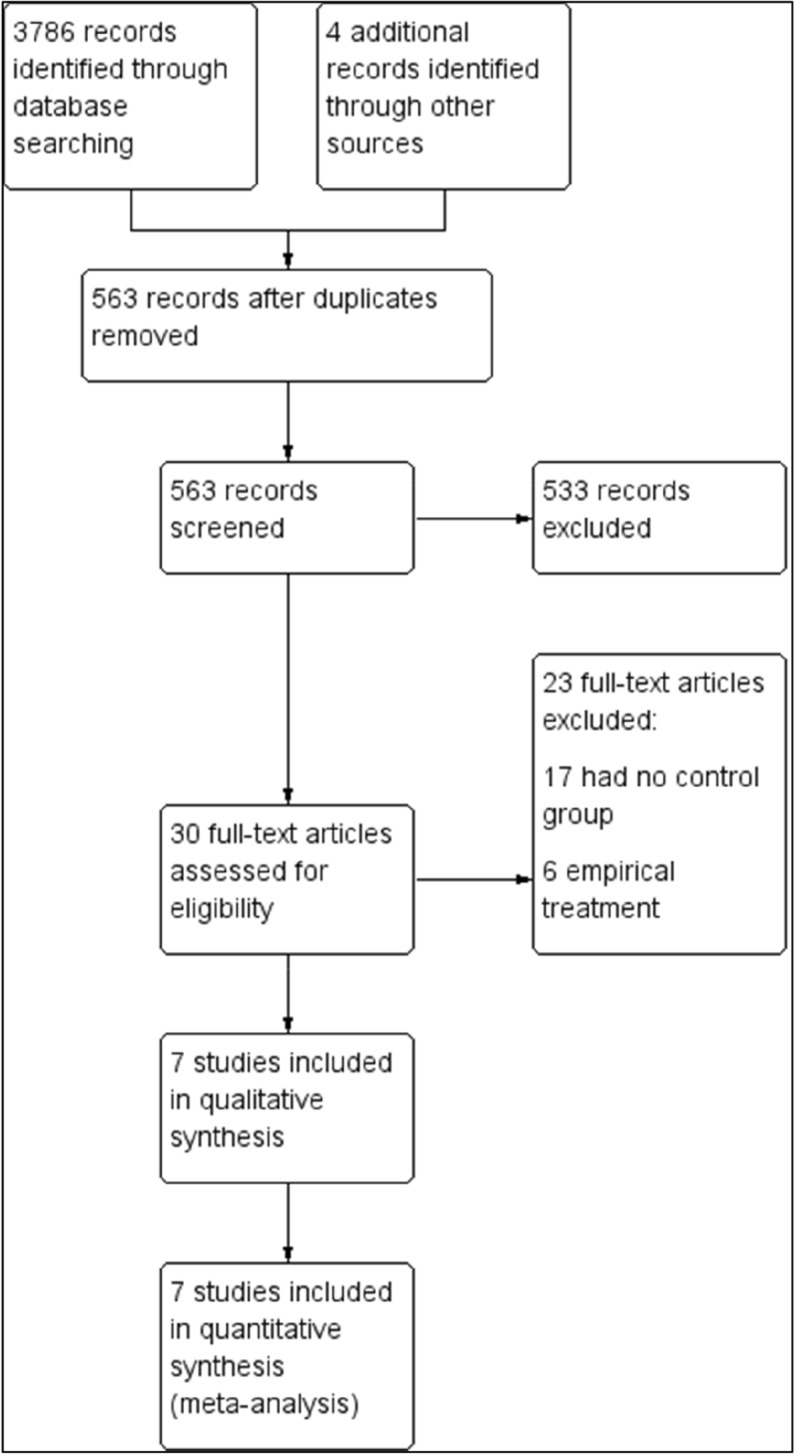
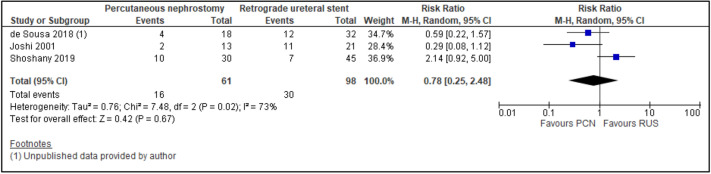
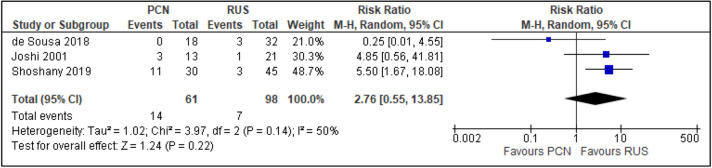
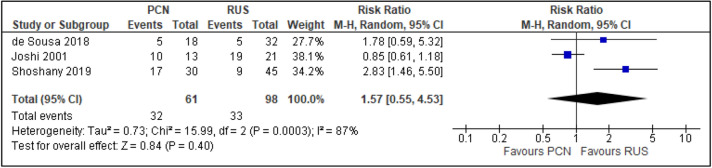
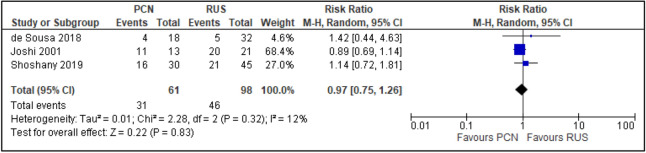
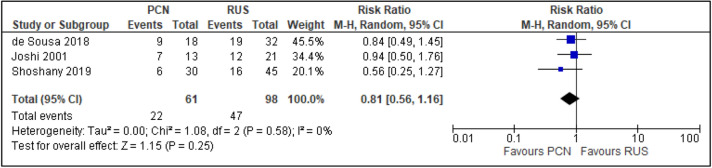
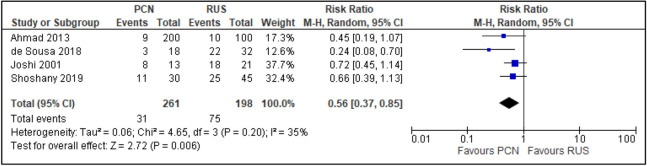
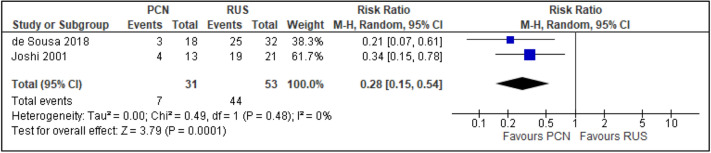
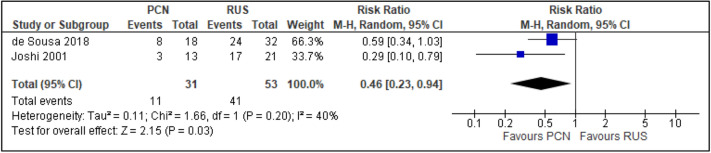
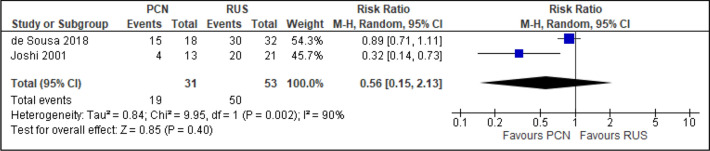
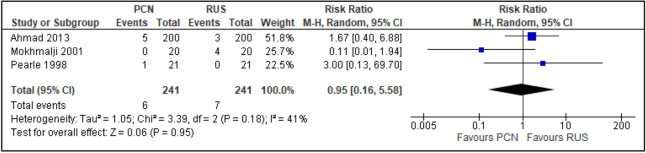
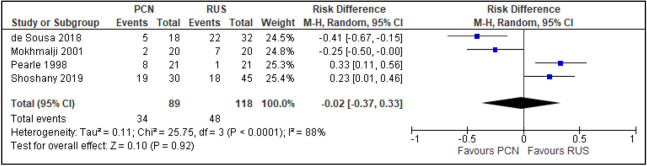
Acute obstructive uropathy is associated with significant morbidity among patients with any condition that leads to urinary tract obstruction. Immediate urinary diversion is necessary to prevent further damage to the kidneys. In many centres, the two main treatment options include percutaneous nephrostomy (PCN) and retrograde ureteral stenting (RUS). The purpose of this study if to compare the efficacy and safety of PCN and RUS for the treatment of acute obstructive uropathy. We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, CINAHL, EMBASE, the World Health Organisation International Clinical Trials Registry Platform and ClinicalTrials.gov. We also searched the reference lists of included studies to identify any additional trials. We included randomised controlled trials and controlled clinical trials comparing the outcomes of clinical improvement (septic parameters), hospitalisation duration, quality of life, urinary-related symptoms, failure rates, post-procedural pain [measured using a visual analogue scale (VAS)] and analgesics use. We conducted statistical analyses using random effects models and expressed the results as risk ratio (RR) and risk difference (RD) for dichotomous outcomes and mean difference (MD) for continuous outcomes, with 95% confidence intervals (CIs). Seven trials were identified that included 667 patients. Meta-analysis of the data revealed no difference in the two methods in improvement of septic parameters, quality of life, failure rates, post-procedural pain (VAS), or analgesics use. Patients receiving PCN had lower rates of haematuria and dysuria post-operatively and longer hospitalisation duration than those receiving RUS. PCN and RUS are effective for the decompression of an obstructed urinary system, with no significant difference in most outcomes. However, PCN is preferable to RUS because of its reduced impact on the patient's post-operative quality of life due to haematuria and dysuria, although it is associated with slightly longer hospitalisation duration.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Khan, A., et al. Epidemiology of chronic kidney disease in an adult Malaysian population (2014).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
