

Prediction of Mortality Using Different COPD Risk Assessments - A 12-Year Follow-Up
- PMID: 33758503
- PMCID: PMC7981171
- DOI: 10.2147/COPD.S282694
Prediction of Mortality Using Different COPD Risk Assessments - A 12-Year Follow-Up
Abstract
Purpose: A multidimensional approach in the risk assessment of chronic obstructive pulmonary disease (COPD) is preferable. The aim of this study is to compare the prognostic ability for mortality by different COPD assessment systems; spirometric staging, classification by GOLD 2011, GOLD 2017, the age, dyspnea, obstruction (ADO) and the dyspnea, obstruction, smoking, exacerbation (DOSE) indices.
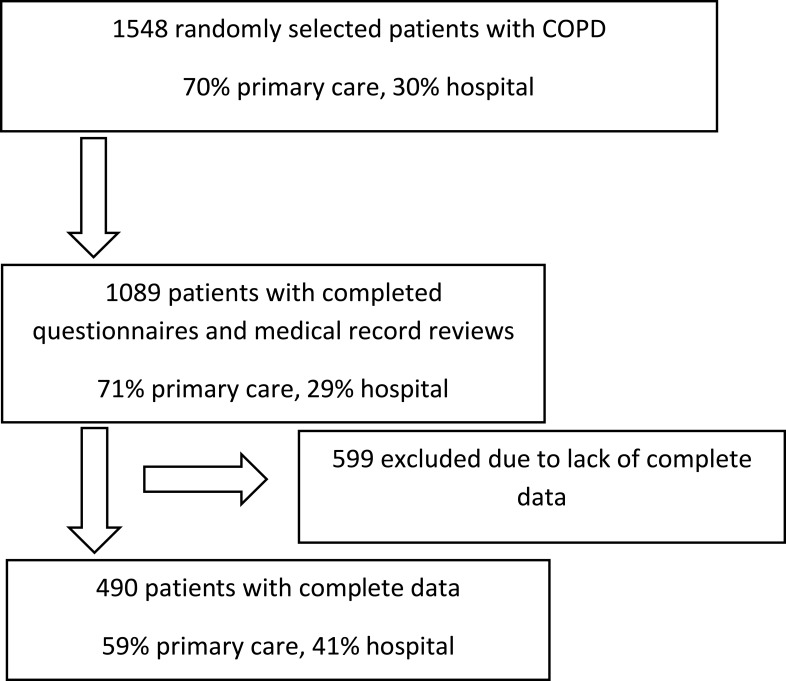
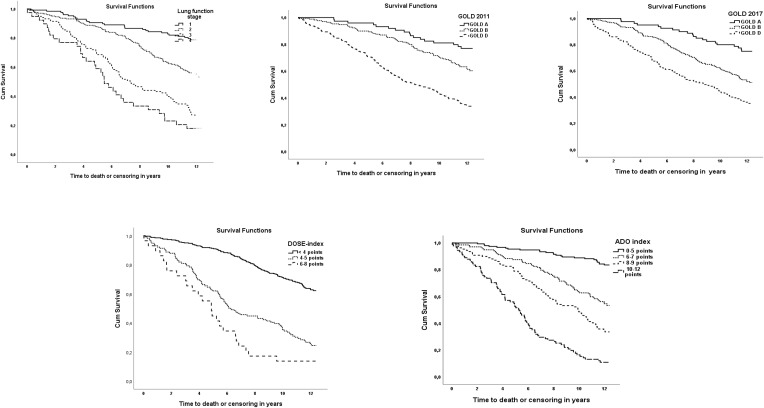
Patients and methods: A total of 490 patients diagnosed with COPD were recruited from primary and secondary care in central Sweden in 2005. The cohort was followed until 2017. Data for categorization using the different assessment systems were obtained through questionnaire data from 2005 and medical record reviews between 2000 and 2003. Kaplan-Meier survival analyses and Cox proportional hazard models were used to assess mortality risk. Receiver operating characteristic curves estimated areas under the curve (AUC) to evaluate each assessment systems´ ability to predict mortality.
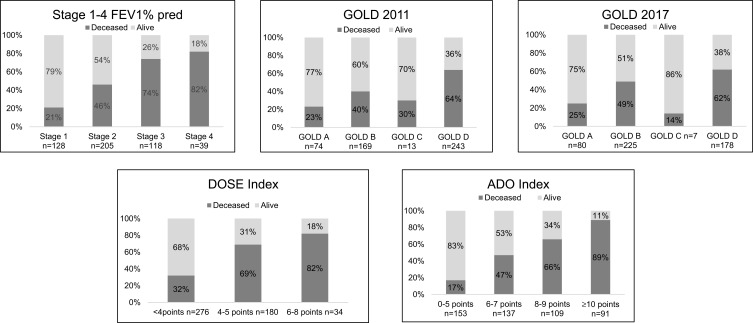
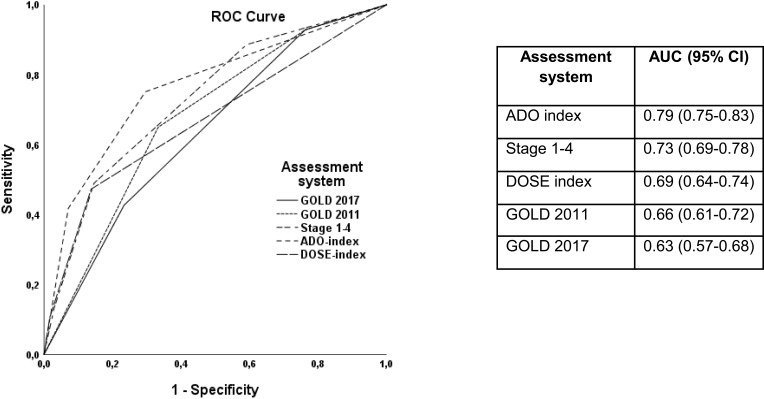
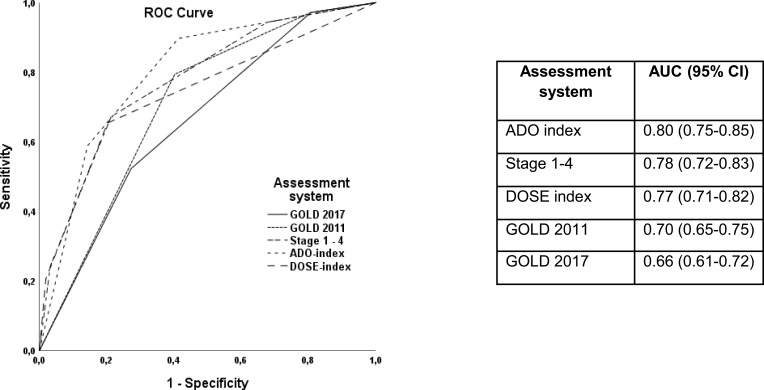
Results: By the end of follow-up, 49% of the patients were deceased. The mortality rate was higher for patients categorized as stage 3-4, GOLD D in both GOLD classifications and those with a DOSE score above 4 and ADO score above 8. The ADO index was most accurate for predicting mortality, AUC 0.79 (95% CI 0.75-0.83) for all-cause mortality and 0.80 (95% CI 0.75-0.85) for respiratory mortality. The AUC values for stages 1-4, GOLD 2011, GOLD 2017 and DOSE index were 0.73, 0.66, 0.63 and 0.69, respectively, for all-cause mortality.
Conclusion: All of the risk assessment systems predict mortality. The ADO index was in this study the best predictor and could be a helpful tool in COPD risk assessment.
Keywords: ADO index; DOSE index; GOLD classification; chronic obstructive pulmonary disease; mortality; prediction.
© 2021 Athlin et al.
Conflict of interest statement
Dr Karin Lisspers reports personal fees from Payments for lectures and educational activities, personal fees from Advisory board, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Multi-component assessment of chronic obstructive pulmonary disease: an evaluation of the ADO and DOSE indices and the global obstructive lung disease categories in international primary care data sets.NPJ Prim Care Respir Med. 2016 Apr 7;26:16010. doi: 10.1038/npjpcrm.2016.10. NPJ Prim Care Respir Med. 2016. PMID: 27053297 Free PMC article.
-
Validation of the GOLD 2017 and new 16 subgroups (1A-4D) classifications in predicting exacerbation and mortality in COPD patients.Int J Chron Obstruct Pulmon Dis. 2018 Oct 18;13:3425-3433. doi: 10.2147/COPD.S179048. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 30425472 Free PMC article.
-
The Ability of Different Scoring Systems to Predict Mortality in Chronic Obstructive Pulmonary Disease Patients: A Prospective Cohort Study.Respiration. 2019;98(6):495-502. doi: 10.1159/000502826. Epub 2019 Oct 30. Respiration. 2019. PMID: 31665736
-
Predictive properties of different multidimensional staging systems in patients with chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2011;6:521-6. doi: 10.2147/COPD.S24420. Epub 2011 Oct 11. Int J Chron Obstruct Pulmon Dis. 2011. PMID: 22069363 Free PMC article.
-
Multidimensional indices in the assessment of chronic obstructive pulmonary disease.Respir Med. 2021 Aug-Sep;185:106519. doi: 10.1016/j.rmed.2021.106519. Epub 2021 Jun 22. Respir Med. 2021. PMID: 34175803 Review.
Cited by
-
Comparison of BODE and ADO Indices in Predicting COPD-Related Medical Costs.Medicina (Kaunas). 2023 Mar 15;59(3):577. doi: 10.3390/medicina59030577. Medicina (Kaunas). 2023. PMID: 36984578 Free PMC article.
-
The DOSE index in chronic obstructive pulmonary disease: evaluating healthcare costs.BMC Pulm Med. 2024 Nov 8;24(1):560. doi: 10.1186/s12890-024-03368-0. BMC Pulm Med. 2024. PMID: 39516765 Free PMC article.
-
RiskPath: Explainable deep learning for multistep biomedical prediction in longitudinal data.medRxiv [Preprint]. 2024 Dec 26:2024.09.19.24313909. doi: 10.1101/2024.09.19.24313909. medRxiv. 2024. Update in: Patterns (N Y). 2025 Apr 28;6(8):101240. doi: 10.1016/j.patter.2025.101240. PMID: 39371168 Free PMC article. Updated. Preprint.
-
The Impact of the Age, Dyspnoea, and Airflow Obstruction (ADO) Index on the Medical Burden of Chronic Obstructive Pulmonary Disease (COPD).J Clin Med. 2022 Mar 29;11(7):1893. doi: 10.3390/jcm11071893. J Clin Med. 2022. PMID: 35407503 Free PMC article.
-
RiskPath: Explainable deep learning for multistep biomedical prediction in longitudinal data.Patterns (N Y). 2025 Apr 28;6(8):101240. doi: 10.1016/j.patter.2025.101240. eCollection 2025 Aug 8. Patterns (N Y). 2025. PMID: 40843347 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
