

Adherence to Multidrug Resistant Tuberculosis Treatment and Case Management in Chongqing, China - A Mixed Method Research Study
- PMID: 33758516
- PMCID: PMC7979342
- DOI: 10.2147/IDR.S293583
Adherence to Multidrug Resistant Tuberculosis Treatment and Case Management in Chongqing, China - A Mixed Method Research Study
Abstract
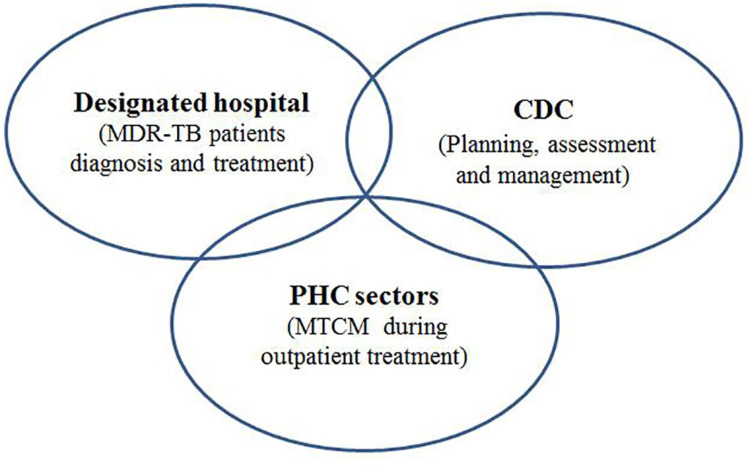
Aim: This paper evaluated the treatment adherence for multidrug-resistant tuberculosis (MDR-TB) and MDR-TB case management (MTCM) in Chongqing, China in order to identify factors associated with poor treatment adherence and case management.
Methods: Surveys with 132 MDR-TB patients and six in-depth interviews with health care workers (HCWs) from primary health centers (PHC), doctors from MDR-TB designated hospitals and MDR-TB patients were conducted. Surveys collected demographic and socio-economic characteristics, as well as factors associated with treatment and case management. In-depth interviews gathered information on treatment and case management experience and adherence behaviors.
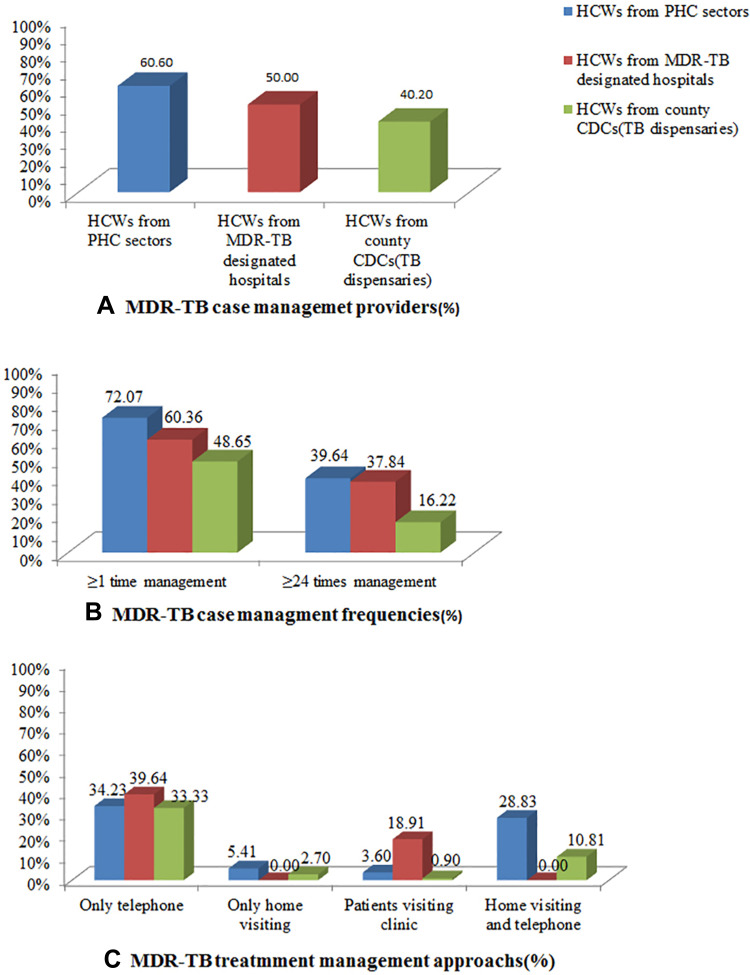
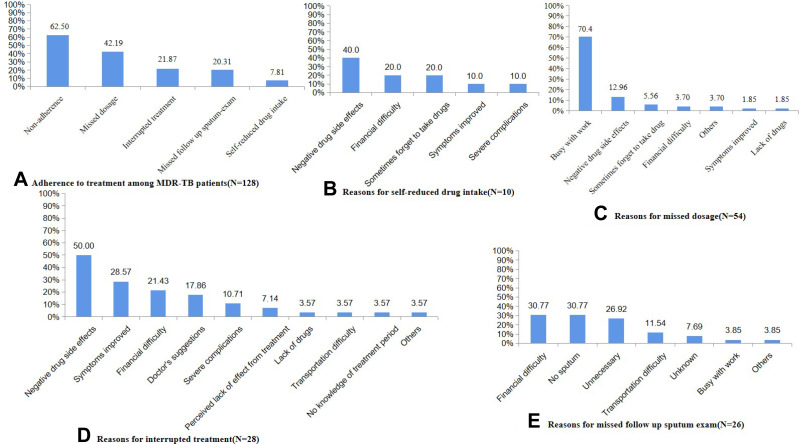
Results: Patient surveys found the two main reasons for poor adherence were negative side-effects from the treatment and busy work schedules. In-depth interviews with key stakeholders found that self-perceived symptom improvement, negative side-effects from treatment and financial difficulties were the main reasons for poor adherence. MDR-TB patients from urban areas, who were unmarried, were female, had migrant status, and whose treatments were supervised by health care workers from primary health clinics, had poorer treatment adherence (P<0.05). Among the MDR-TB patients surveyed, 86.7% received any type of MTCM in general (received any kind of MTCM from HCWs in PHC, MDR-TB designated hospital and centers of disease control/TB dispensaries and 62.50% received MTCM from HCWs in PHC sectors). Patients from suburban areas were more likely to receive both MTCM in general (OR=6.70) and MTCM from HCWs in MDR-TB designated hospitals (OR=2.77), but female patients (OR=0.26) were less likely to receive MTCM from HCWs in PHC sectors, and patients who were not educated about MTCM by TB doctors in designated hospitals were less likely to receive MTCM in general (OR=0.14). Patients who had not been hospitalized were less likely to receive MTCM from HCWs in MDR-TB designated hospitals (OR=0.21).
Conclusion: Stronger MTCM by HCWs in PHC sectors would improve treatment adherence among MDR-TB patients. Community-based patient-centered models of MTCM in PHC sectors and the use of digital health technology could help to improve case management and thereby improve adherence.
Keywords: adherence behaviors; management; multi-drug-resistant tuberculosis; treatment.
© 2021 Xing et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Implementation factors of tuberculosis control program in primary healthcare settings in China: a mixed-methods using the Consolidated Framework for Implementation Research framework.Infect Dis Poverty. 2024 Jul 8;13(1):52. doi: 10.1186/s40249-024-01222-3. Infect Dis Poverty. 2024. PMID: 38978081 Free PMC article.
-
Challenge of ending TB in China: tuberculosis control in primary healthcare sectors under integrated TB control model-a systematic review and meta-analysis.BMC Public Health. 2024 Jan 11;24(1):163. doi: 10.1186/s12889-023-16292-5. BMC Public Health. 2024. PMID: 38212753 Free PMC article.
-
The job burnout of tuberculosis healthcare workers and associated factors under integrated tuberculosis control model: a mixed-method study based on the two-factor theory.BMC Health Serv Res. 2024 Aug 26;24(1):984. doi: 10.1186/s12913-024-11472-4. BMC Health Serv Res. 2024. PMID: 39187887 Free PMC article.
-
Tuberculosis treatment management in primary healthcare sectors: a mixed-methods study investigating delivery status and barriers from organisational and patient perspectives.BMJ Open. 2022 Apr 20;12(4):e053797. doi: 10.1136/bmjopen-2021-053797. BMJ Open. 2022. PMID: 35443945 Free PMC article.
-
Risk factors of multidrug-resistant tuberculosis in China: A meta-analysis.Public Health Nurs. 2019 May;36(3):257-269. doi: 10.1111/phn.12582. Epub 2019 Jan 24. Public Health Nurs. 2019. PMID: 30680796
Cited by
-
A conceptual framework on determinants of the integrated tuberculosis control model implementation in China.Front Med (Lausanne). 2024 Aug 21;11:1407131. doi: 10.3389/fmed.2024.1407131. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39234037 Free PMC article.
-
Implementation factors of tuberculosis control program in primary healthcare settings in China: a mixed-methods using the Consolidated Framework for Implementation Research framework.Infect Dis Poverty. 2024 Jul 8;13(1):52. doi: 10.1186/s40249-024-01222-3. Infect Dis Poverty. 2024. PMID: 38978081 Free PMC article.
-
Development and validation of self-management scale for tuberculosis patients.BMC Infect Dis. 2022 May 27;22(1):502. doi: 10.1186/s12879-022-07483-3. BMC Infect Dis. 2022. PMID: 35624424 Free PMC article.
-
Integrating narrative and bibliometric approaches to examine factors and impacts of tuberculosis treatment non-compliance.Multidiscip Respir Med. 2025 Feb 28;20(1):1016. doi: 10.5826/mrm.2025.1016. Multidiscip Respir Med. 2025. PMID: 40017294 Free PMC article.
-
Challenge of ending TB in China: tuberculosis control in primary healthcare sectors under integrated TB control model-a systematic review and meta-analysis.BMC Public Health. 2024 Jan 11;24(1):163. doi: 10.1186/s12889-023-16292-5. BMC Public Health. 2024. PMID: 38212753 Free PMC article.
References
-
- WHO. Global Tuberculosis Report, 2020. Geneva: World Health Organization; July, 2020. Available from: https://www.who.int/. Accessed February25, 2021.
-
- WHO. The End TB Strategy. Geneva: World Health Organization; 2014. Available from: https://www.who.int/. Accessed July, 2020.
-
- Cheng SM. Current situation and recommendation of MDR-TB prevention and control in China. China Trop Med. 2017;17(3):213–215.
LinkOut - more resources
Full Text Sources
Other Literature Sources
