

COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis
- PMID: 33758801
- PMCID: PMC7971471
- DOI: 10.1016/j.eclinm.2021.100789
COPD and the risk of poor outcomes in COVID-19: A systematic review and meta-analysis
Abstract
Background: Patients with chronic obstructive pulmonary disease (COPD) are highly susceptible from respiratory exacerbations from viral respiratory tract infections. However, it is unclear whether they are at increased risk of COVID-19 pneumonia or COVID-19-related mortality. We aimed to determine whether COPD is a risk factor for adverse COVID-19 outcomes including hospitalization, severe COVID-19, or death.
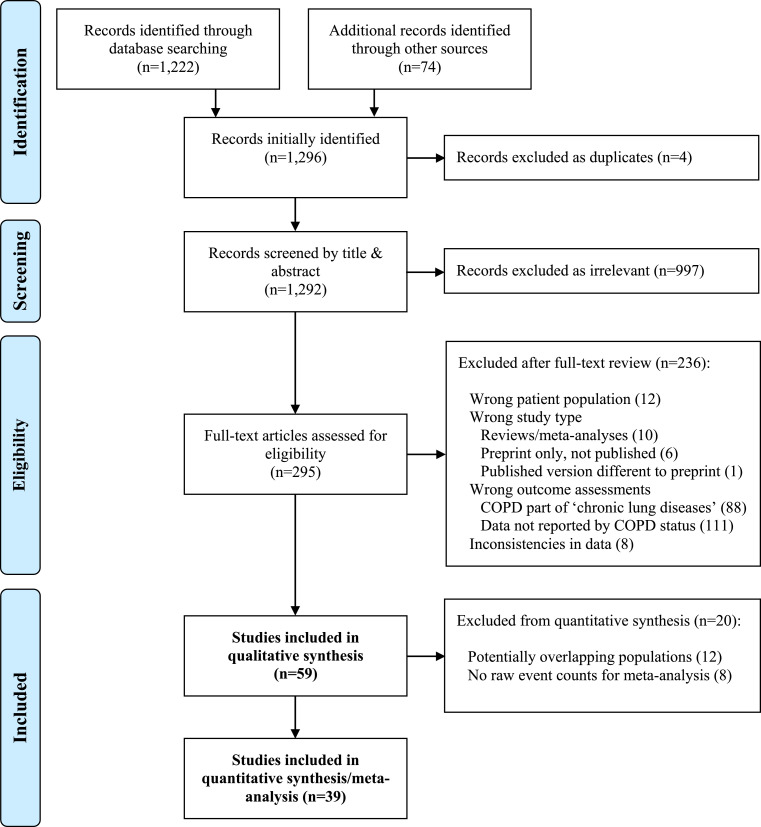
Methods: Following the PRISMA guidelines, we performed a systematic review of COVID-19 clinical studies published between November 1st, 2019 and January 28th, 2021 (PROSPERO ID: CRD42020191491). We included studies that quantified the number of COPD patients, and reported at least one of the following outcomes stratified by COPD status: hospitalization; severe COVID-19; ICU admission; mechanical ventilation; acute respiratory distress syndrome; or mortality. We meta-analyzed the results of individual studies to determine the odds ratio (OR) of these outcomes in patients with COPD compared to those without COPD.
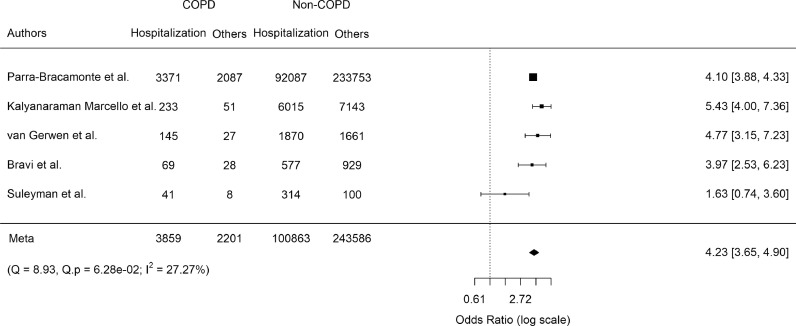
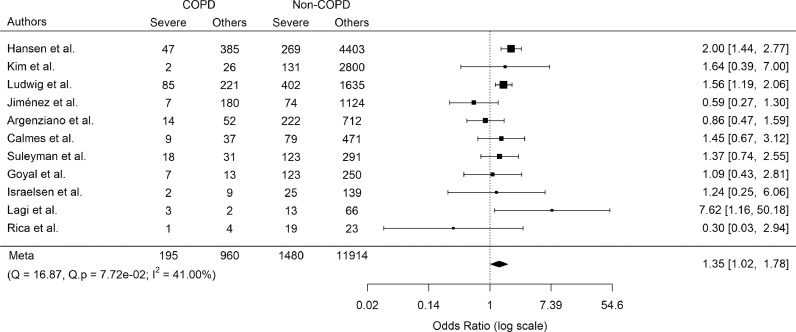
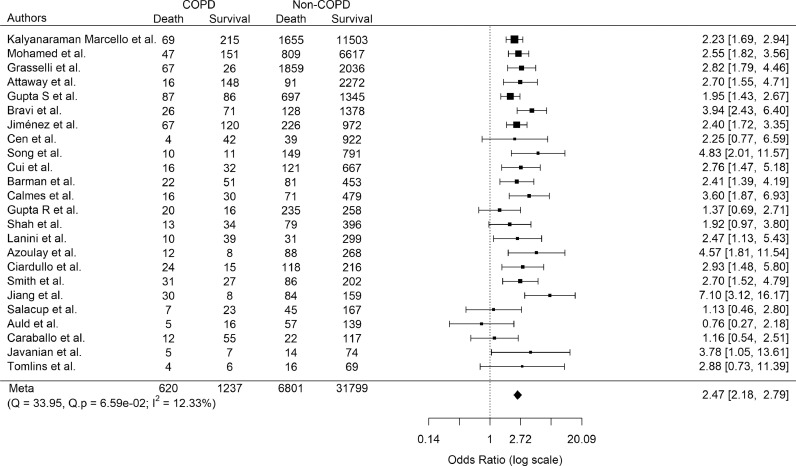
Findings: Fifty-nine studies met the inclusion criteria, and underwent data extraction. Most studies were retrospective cohort studies/case series of hospitalized patients. Only four studies examined the effects of COPD on COVID-19 outcomes as their primary endpoint. In aggregate, COPD was associated with increased odds of hospitalization (OR 4.23, 95% confidence interval [CI] 3.65-4.90), ICU admission (OR 1.35, 95% CI 1.02-1.78), and mortality (OR 2.47, 95% CI 2.18-2.79).
Interpretation: Having a clinical diagnosis of COPD significantly increases the odds of poor clinical outcomes in patients with COVID-19. COPD patients should thus be considered a high-risk group, and targeted for preventative measures and aggressive treatment for COVID-19 including vaccination.
Keywords: COPD; COVID-19; Meta-analysis; mortality.
© 2021 The Authors.
Conflict of interest statement
SM reports personal fees from Novartis and Boehringer-Ingelheim, outside the submitted work. DDS reports grants and personal fees from AstraZeneca, personal fees from Boehringer Ingelheim, and personal fees from Grifols outside the submitted work. FVG, CC, XL, CWTY, AT, LC, and AB have nothing to disclose.
Figures
References
-
- Johns Hopkins University and Medical Center . 2021. Johns Hopkins coronavirus resource center.https://coronavirus.jhu.edu [online resource]. Available at. [last accessed 11 February]
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
