

Describing the Weight-Reduced State: Physiology, Behavior, and Interventions
- PMID: 33759395
- PMCID: PMC9022199
- DOI: 10.1002/oby.23086
Describing the Weight-Reduced State: Physiology, Behavior, and Interventions
Abstract
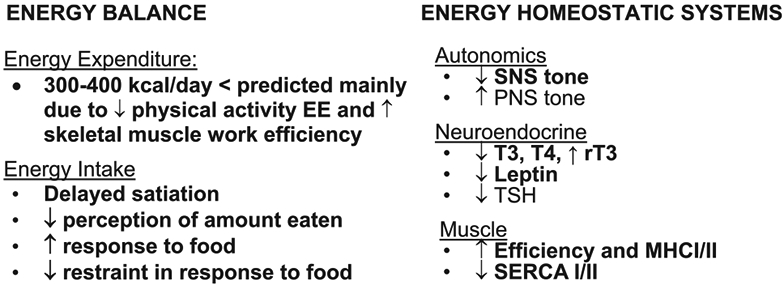
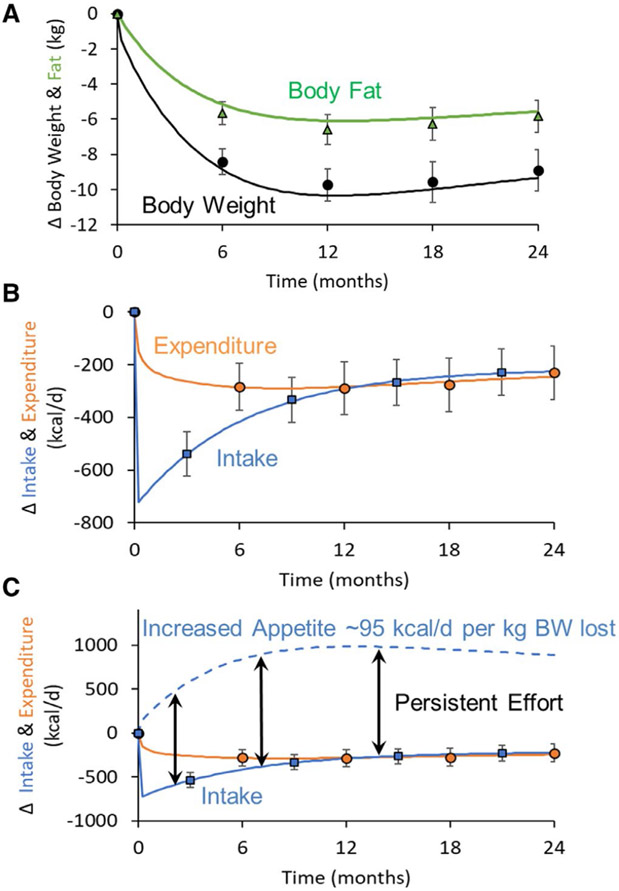
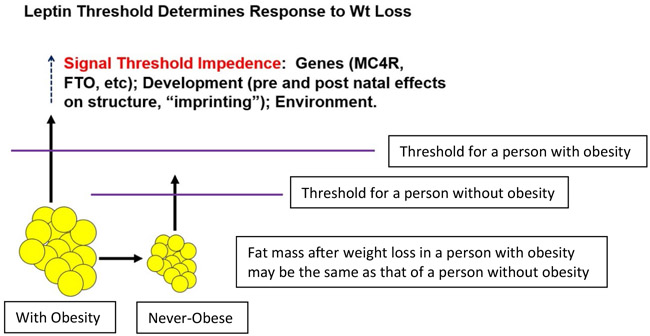
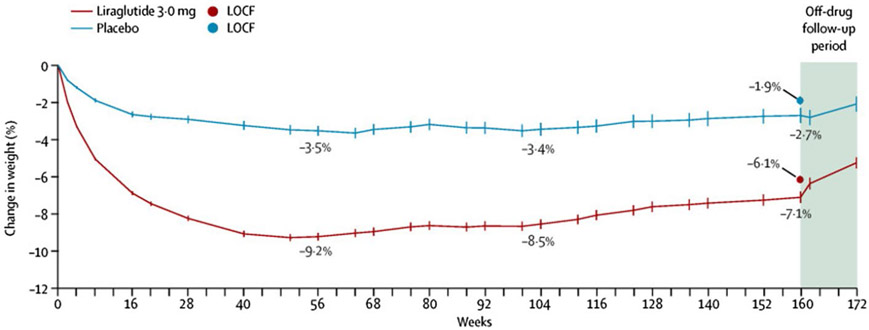
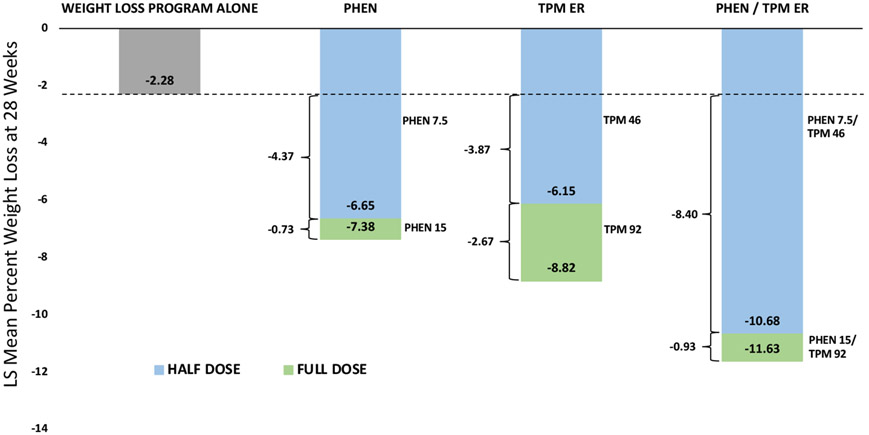
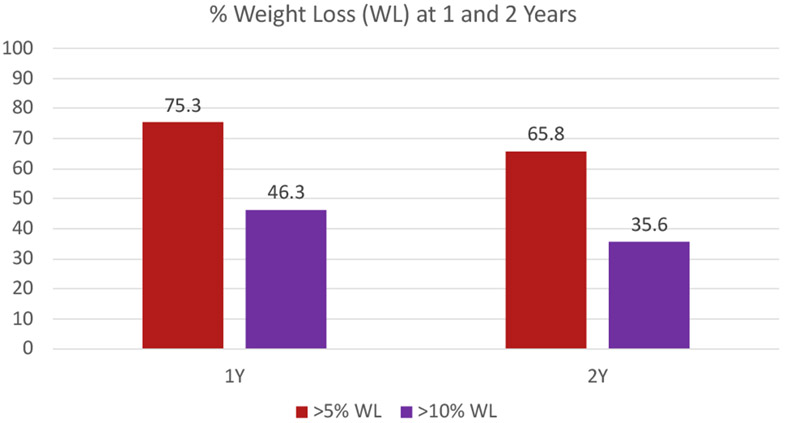
Although many persons with obesity can lose weight by lifestyle (diet and physical activity) therapy, successful long-term weight loss is difficult to achieve, and most people who lose weight regain their lost weight over time. The neurohormonal, physiological, and behavioral factors that promote weight recidivism are unclear and complex. The National Institute of Diabetes and Digestive and Kidney Diseases convened a workshop in June 2019, titled "The Physiology of the Weight-Reduced State," to explore the mechanisms and integrative physiology of adaptations in appetite, energy expenditure, and thermogenesis that occur in the weight-reduced state and that may oppose weight-loss maintenance. The proceedings from the first session of this workshop are presented here. Drs. Michael Rosenbaum, Kevin Hall, and Rudolph Leibel discussed the physiological factors that contribute to weight regain; Dr. Michael Lowe discussed the biobehavioral issues involved in weight-loss maintenance; Dr. John Jakicic discussed the influence of physical activity on long-term weight-loss maintenance; and Dr. Louis Aronne discussed the ability of drug therapy to maintain weight loss.
© 2021 The Obesity Society.
Conflict of interest statement
Figures
Comment in
-
Recidivism: An artifact of implicit weight bias in obesity research.Obesity (Silver Spring). 2021 Aug;29(8):1237. doi: 10.1002/oby.23205. Epub 2021 Jun 14. Obesity (Silver Spring). 2021. PMID: 34128334 No abstract available.
-
Word selection and weight bias.Obesity (Silver Spring). 2021 Aug;29(8):1238. doi: 10.1002/oby.23203. Epub 2021 Jun 14. Obesity (Silver Spring). 2021. PMID: 34128587 No abstract available.
References
-
- Wing R, Phelan S. Long-term weight maintenance. Amer J Clin Nutr 2005;82:222S–225S. - PubMed
-
- Phelan S, Wing R. Prevalance of successful weight loss. Arch Intern Med 2005;165:2430. - PubMed
-
- Thomas J, Bond D, Phelan S, Hill J, Wing R. Weight-loss maintenance for 10 years in the National Weight Control Registry. Am J Prev Med 2014;46:17–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
