

Type 1 diabetes mellitus: much progress, many opportunities
- PMID: 33759815
- PMCID: PMC8262558
- DOI: 10.1172/JCI142242
Type 1 diabetes mellitus: much progress, many opportunities
Abstract
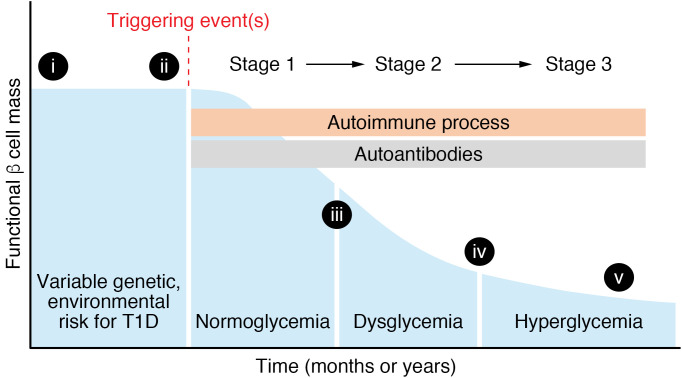
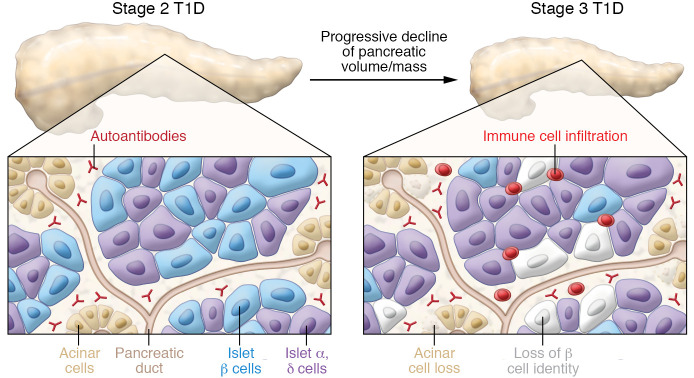
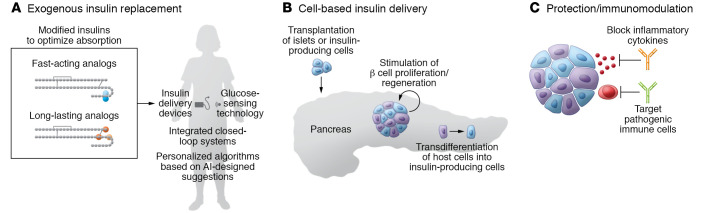
As part of the centennial celebration of insulin's discovery, this review summarizes the current understanding of the genetics, pathogenesis, treatment, and outcomes in type 1 diabetes (T1D). T1D results from an autoimmune response that leads to destruction of the β cells in the pancreatic islet and requires lifelong insulin therapy. While much has been learned about T1D, it is now clear that there is considerable heterogeneity in T1D with regard to genetics, pathology, response to immune-based therapies, clinical course, and susceptibility to diabetes-related complications. This Review highlights knowledge gaps and opportunities to improve the understanding of T1D pathogenesis and outlines emerging therapies to treat or prevent T1D and reduce the burden of T1D.
Conflict of interest statement
Figures
References
-
- Bliss M. The Discovery of Insulin. University of Toronto Press; 1982.
-
- Cooper T, Ainsberg A. Breakthrough: Elizabeth Hughes, the Discovery of Insulin, and the Making of a Medical Miracle. St. Martin’s Publishing Group; 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
