

Comparison of New York Heart Association Class and Patient-Reported Outcomes for Heart Failure With Reduced Ejection Fraction
- PMID: 33760037
- PMCID: PMC7992023
- DOI: 10.1001/jamacardio.2021.0372
Comparison of New York Heart Association Class and Patient-Reported Outcomes for Heart Failure With Reduced Ejection Fraction
Abstract
Importance: It is unclear how New York Heart Association (NYHA) functional class compares with patient-reported outcomes among patients with heart failure (HF) in contemporary US clinical practice.
Objective: To characterize longitudinal changes and concordance between NYHA class and the Kansas City Cardiomyopathy Questionnaire Overall Summary Score (KCCQ-OS), and their associations with clinical outcomes.
Design, setting, and participants: This cohort study included 2872 US outpatients with chronic HF with reduced ejection fraction across 145 practices enrolled in the CHAMP-HF registry between December 2015 and October 2017. All patients had complete NYHA class and KCCQ-OS data at baseline and 12 months. Longitudinal changes and correlations between the 2 measure were examined. Multivariable models landmarked at 12 months evaluated associations between improvement in NYHA and KCCQ-OS from baseline to 12 months with clinical outcomes occurring from months 12 through 24. Statistical analyses were performed from March to August 2020.
Exposure: Change in health status, as defined by 12-month change in NYHA class or KCCQ-OS.
Main outcomes and measures: All-cause mortality, HF hospitalization, and mortality or HF hospitalization.
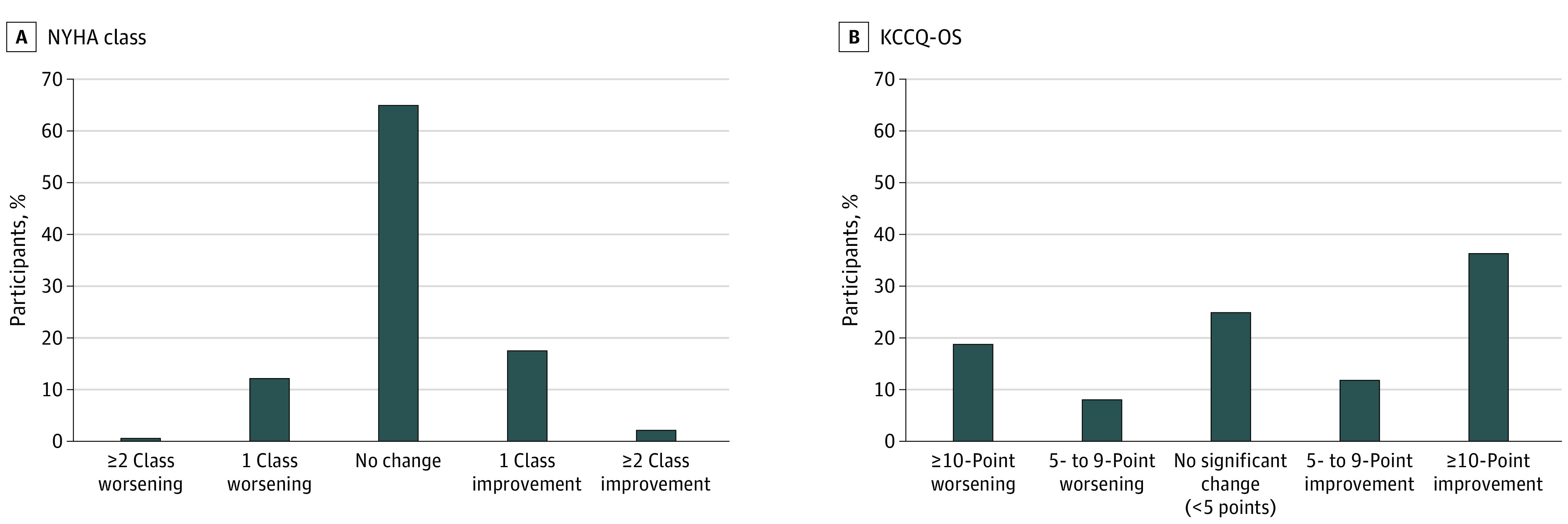
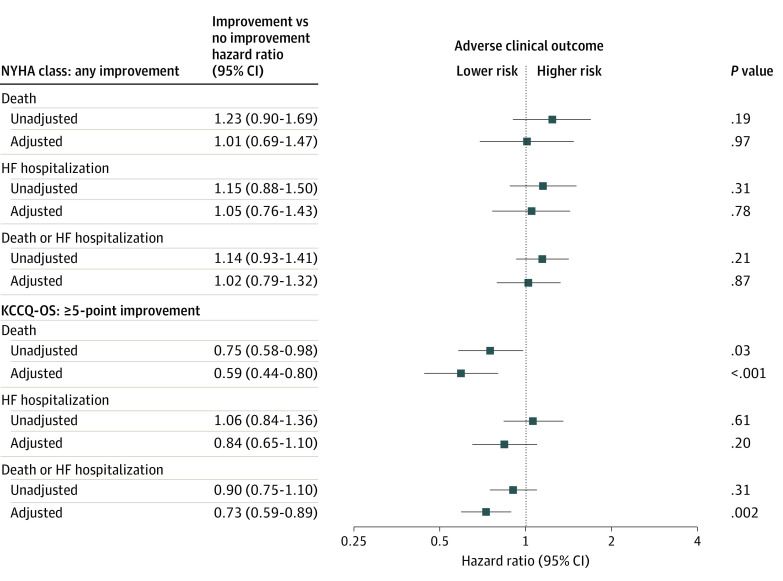
Results: In total, 2872 patients were included in this analysis (median [interquartile range] age, 68 [59-75] years; 872 [30.4%] were women; and 2156 [75.1%] were of White race). At baseline, 312 patients (10.9%) were NYHA class I, 1710 patients (59.5%) were class II, 804 patients (28.0%) were class III, and 46 patients (1.6%) were class IV. For KCCQ-OS, 1131 patients (39.4%) scored 75 to 100 (best health status), 967 patients (33.7%) scored 50 to 74, 612 patients (21.3%) scored 25 to 49, and 162 patients (5.6%) scored 0 to 24 (worst health status). At 12 months, 1002 patients (34.9%) had a change in NYHA class (599 [20.9%] with improvement; 403 [14.0%] with worsening) and 2158 patients (75.1%) had a change of 5 or more points in KCCQ-OS (1388 [48.3%] with improvement; 770 [26.8%] with worsening). The most common trajectory for NYHA class was no change (1870 [65.1%]), and the most common trajectory for KCCQ-OS was an improvement of at least 10 points (1047 [36.5%]). After adjustment, improvement in NYHA class was not associated with subsequent clinical outcomes, whereas an improvement of 5 or more points in KCCQ-OS was independently associated with decreased mortality (hazard ratio, 0.59; 95% CI, 0.44-0.80; P < .001) and mortality or HF hospitalization (hazard ratio, 0.73; 95% CI, 0.59-0.89; P = .002).
Conclusions and relevance: Findings of this cohort study suggest that, in contemporary US clinical practice, compared with NYHA class, KCCQ-OS is more sensitive to clinically meaningful changes in health status over time. Changes in KCCQ-OS may have more prognostic value than changes in NYHA class.
Conflict of interest statement
Figures
Comment in
-
The Growing Case for Routine Collection of Patient-Reported Outcomes.JAMA Cardiol. 2021 May 1;6(5):497-498. doi: 10.1001/jamacardio.2021.0391. JAMA Cardiol. 2021. PMID: 33760011 No abstract available.
References
-
- White PD, Myers MM. The classification of cardiac diagnosis. JAMA. 1921;77(18):1414-1415. doi: 10.1001/jama.1921.02630440034013 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
