

Bridging the age gap in breast cancer: impact of omission of breast cancer surgery in older women with oestrogen receptor-positive early breast cancer on quality-of-life outcomes
- PMID: 33760065
- PMCID: PMC10364859
- DOI: 10.1093/bjs/znaa125
Bridging the age gap in breast cancer: impact of omission of breast cancer surgery in older women with oestrogen receptor-positive early breast cancer on quality-of-life outcomes
Abstract
Background: Primary endocrine therapy may be an alternative treatment for less fit women with oestrogen receptor (ER)-positive breast cancer. This study compared quality-of-life (QoL) outcomes in older women treated with surgery or primary endocrine therapy.
Methods: This was a multicentre, prospective, observational cohort study of surgery or primary endocrine therapy in women aged over 70 years with operable breast cancer. QoL was assessed using European Organisation for Research and Treatment of cancer QoL questionnaires QLQ-C30, -BR23, and -ELD14, and the EuroQol Five Dimensions 5L score at baseline, 6 weeks, and 6, 12, 18, and 24 months. Propensity score matching was used to adjust for baseline variation in health, fitness, and tumour stage.
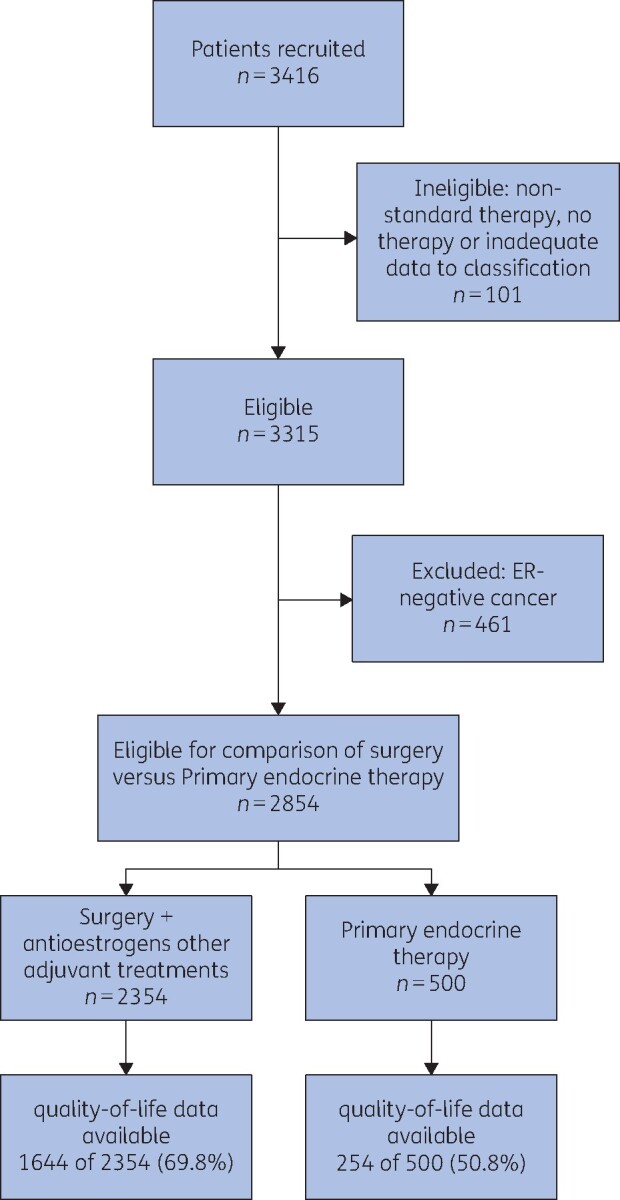
Results: The study recruited 3416 women (median age 77 (range 69-102) years) from 56 breast units. Of these, 2979 (87.2 per cent) had ER-positive breast cancer; 2354 women had surgery and 500 received primary endocrine therapy (125 were excluded from analysis due to inadequate data or non-standard therapy). Median follow-up was 52 months. The primary endocrine therapy group was older and less fit. Baseline QoL differed between the groups; the mean(s.d.) QLQ-C30 global health status score was 66.2(21.1) in patients who received primary endocrine therapy versus 77.1(17.8) among those who had surgery plus endocrine therapy. In the unmatched analysis, changes in QoL between 6 weeks and baseline were noted in several domains, but by 24 months most scores had returned to baseline levels. In the matched analysis, major surgery (mastectomy or axillary clearance) had a more pronounced adverse impact than primary endocrine therapy in several domains.
Conclusion: Adverse effects on QoL are seen in the first few months after surgery, but by 24 months these have largely resolved. Women considering surgery should be informed of these effects.
Antecedentes: : El tratamiento hormonal exclusivo puede ser una alternativa para las mujeres frágiles con cáncer de mama ER +. Este estudio comparó la calidad de vida en mujeres mayores tratadas con cirugía o con tratamiento hormonal como modalidad única.
Métodos: : Estudio prospectivo, multicéntrico, observacional de una cohorte de mujeres de > 70 años de edad con cáncer de mama operable en las que se optó por tratamiento quirúrgico u hormonal exclusivo. Se evaluó la calidad de vida mediante los cuestionarios C30, BR23 y ELD14 de la EORTC y el EQ5D al inicio del estudio y a las 6 semanas y 6, 12, 18 y 24 meses. Se realizó un estudio de emparejamiento por puntaje de propensión para ajustar el estado general y físico basal y el estadio del tumor.
Resultados: : Se reclutaron 3.416 mujeres (mediana de edad 77 años, rango 69-102) en 56 unidades de mama. La mediana de seguimiento fue de 52 meses. Un total de 2.979 (88%) mujeres padecian un cáncer de mama ER + y se trataron mediante cirugía 2.354 y 500 con tratamiento hormonal. El grupo que recibió úncamente tratamiento hormonal era mayor y más frágil. La calidad de vida inicial varió entre ambos grupos; la puntuación media en el cuestionario de salud general C30 fue de 66,2 (desviación estándar, DE 21,1) en el grupo con tratamiento hormonal exclusivo frente a 77,1 (DE 17,8) en el grupo con cirugía y tratamiento endocrino. En el análisis de toda la serie, se observaron diferencias en la calidad de vida en varios dominios en la comparación entre los valores a las 6 semanas y los valores basales, pero a los 24 meses la mayoría de dichos valores habían vuelto a los niveles basales. Tras el emparejamiento, la cirugía mayor (mastectomía o vaciamiento ganglionar) conllevó efectos adversos más graves que el tratamiento hormonal exclusivo en varios dominios.
Conclusión: nque tras la cirugía se observa un deterioro de la calidad de vida en los primeros meses, este deterioro desaparece en gran medida a los 24 meses. Las mujeres que estén considerando la cirugía deben ser informadas de estos efectos.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures




References
-
- Derks MGM, Bastiaannet E, Kiderlen M, Hilling DE, Boelens PG, Walsh PM et al. Variation in treatment and survival of older patients with non-metastatic breast cancer in five European countries: a population-based cohort study from the EURECCA Breast Cancer Group. Br J Cancer 2018; 119:121–129 - PMC - PubMed
-
- Husain LS, Collins K, Reed M, Wyld L. Choices in cancer treatment: a qualitative study of the older women’s (>70 years) perspective. Psychooncology 2008;17:410–416 - PubMed
-
- Biganzoli L, Wildiers H, Oakman C, Marotti L, Loibl S, Kunkler I et al. Management of elderly patients with breast cancer: updated recommendations of the International Society of Geriatric Oncology (SIOG) and European Society of Breast Cancer Specialists (EUSOMA). Lancet Oncol 2012;13:e148–e160 - PubMed
-
- Fallowfield L. Quality of life in the elderly woman with breast cancer treated with tamoxifen and surgery or tamoxifen alone. Journal of Womens Health 1994;3:17–20
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
