

Effect of Behaviorally Designed Gamification With a Social Support Partner to Increase Mobility After Hospital Discharge: A Randomized Clinical Trial
- PMID: 33760089
- PMCID: PMC7991973
- DOI: 10.1001/jamanetworkopen.2021.0952
Effect of Behaviorally Designed Gamification With a Social Support Partner to Increase Mobility After Hospital Discharge: A Randomized Clinical Trial
Abstract
Importance: Hospitalization is associated with decreased mobility and functional decline. Behaviorally designed gamification can increase mobility in community settings but has not been tested among patients at risk for functional decline during a high-risk transition period after hospitalization.
Objective: To test a behaviorally designed gamification intervention with a social support partner to increase patient mobility after hospital discharge.
Design, setting, and participants: This study is a randomized clinical trial of a 12-week intervention without follow-up. Enrollment occurred from January 2018 to June 2019 at a referral hospital with a remote at-home monitoring intervention among patients living predominantly in 3 states (Pennsylvania, New Jersey, and Delaware). Participants included adult patients discharged from general medicine and oncology units to home. Data analysis was performed from October 2019 to March 2020.
Interventions: All participants received a wearable device to track daily steps. The control group received feedback from the device but no other interventions. The intervention group entered into a 12-week game informed by behavioral economics to assign points and levels for achieving step goals and reinforced by a support partner who received updates on participant progress.
Main outcomes and measures: The primary outcome was change in mean daily steps from baseline through the 12-week intervention. Secondary measures were change in functional status and urgent care utilization (ie, emergency department visits and hospital readmissions) within this period.
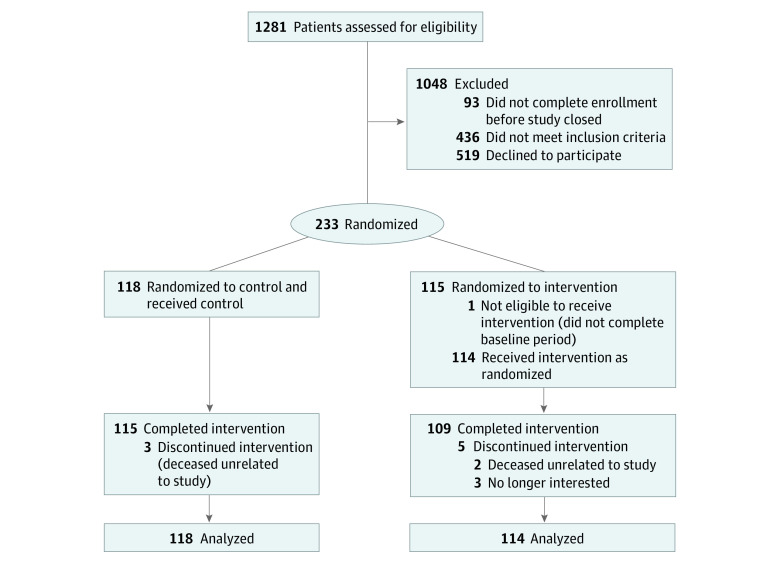
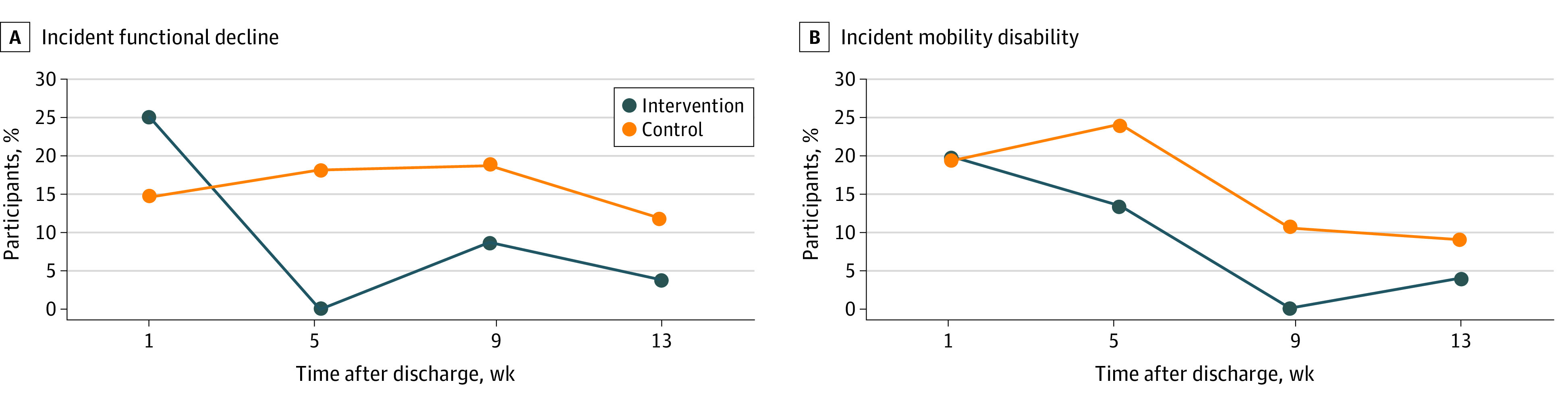
Results: A total of 232 participants were enrolled in the study (118 randomized to control and 114 randomized to the intervention). Participants had a mean (SD) age of 40 (14) years, 141 (61%) were female, 101 (43%) were White, and 103 (44%) had an annual household income less than $50 000. Daily step counts increased from 3795 to 4652 steps (difference, 857 steps; 95% CI, 488 to 1224 steps) among intervention participants and increased from 3951 to 4499 steps (difference, 548 steps; 95% CI, 193 to 903 steps) among control participants. The change in mean daily step count from baseline was not significantly different for participants in the intervention group vs the control group (adjusted difference, 270 steps; 95% CI, -214 to 754 steps; P = .27). Among the subgroup of 76 participants with higher levels of social engagement, post hoc exploratory analyses showed a significant increase in mobility for intervention vs control (adjusted difference, 1125 steps; 95% CI, 409 to 1841 steps; P = .002). Fewer participants in this subgroup experienced functional decline (1 of 36 participants [4%] in the intervention group vs 5 of 40 participants [12%] in the control group) and hospital readmission at 30 days (3 of 36 participants [8%] in the intervention group vs 6 of 40 participants [15%] in the control group), but the differences were not statistically significant. There were no significant differences in these secondary outcomes for the overall sample.
Conclusions and relevance: Gamification with social incentives did not affect mobility or functional decline in all participants, but post hoc analysis suggests positive findings for both outcomes for patients with higher social engagement.
Trial registration: ClinicalTrials.gov Identifier: NCT03321279.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
