

Insight into the roles of melatonin in bone tissue and bone‑related diseases (Review)
- PMID: 33760138
- PMCID: PMC7979260
- DOI: 10.3892/ijmm.2021.4915
Insight into the roles of melatonin in bone tissue and bone‑related diseases (Review)
Abstract
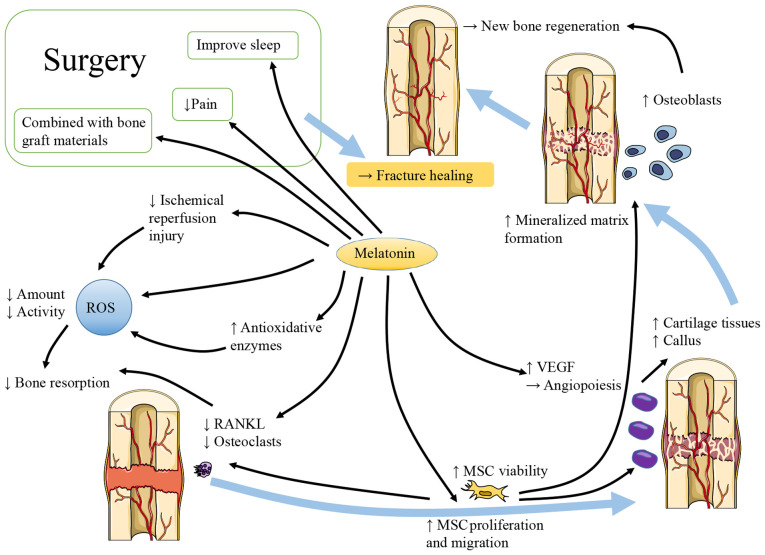
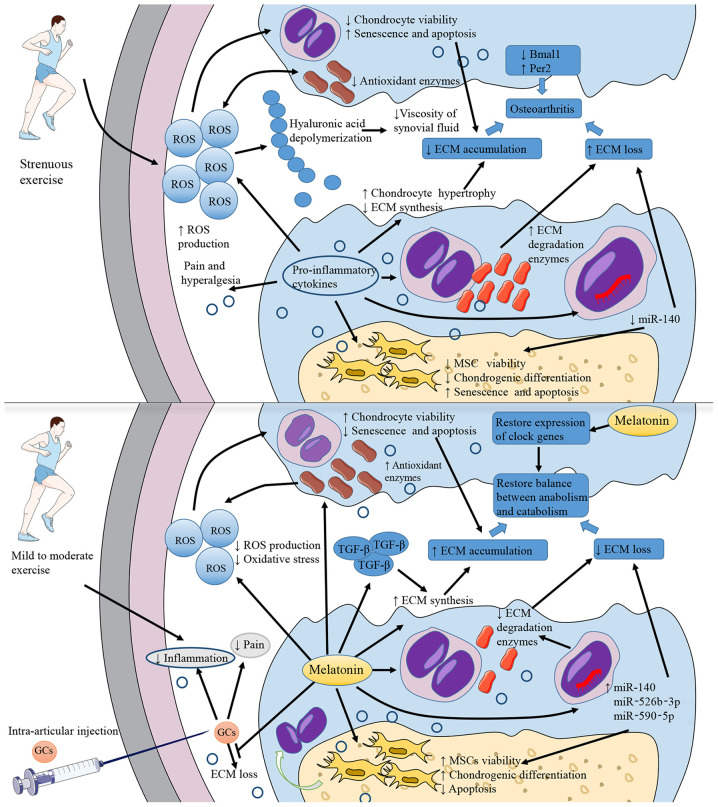
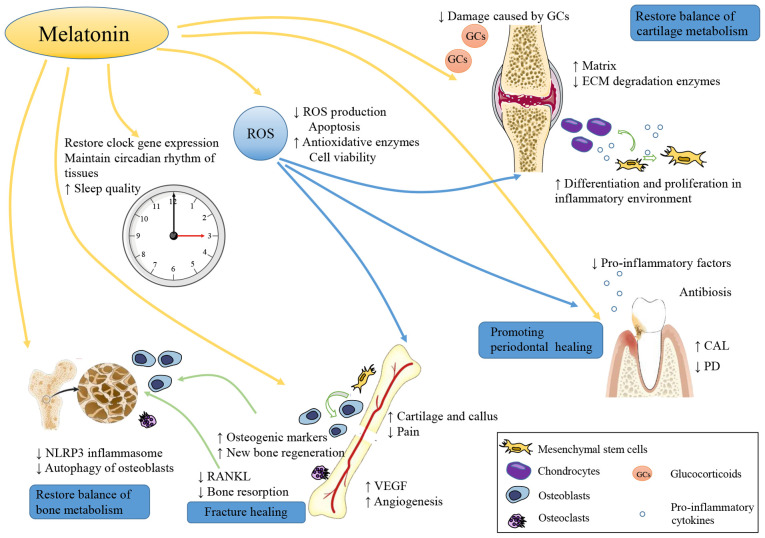
Bone‑related diseases comprise a large group of common diseases, including fractures, osteoporosis and osteoarthritis (OA), which affect a large number of individuals, particularly the elderly. The progressive destruction and loss of alveolar bone caused by periodontitis is a specific type of bone loss, which has a high incidence and markedly reduces the quality of life of patients. With the existing methods of prevention and treatment, the incidence and mortality of bone‑related diseases are still gradually increasing, creating a significant financial burden to societies worldwide. To prevent the occurrence of bone‑related diseases, delay their progression or reverse the injuries they cause, new alternative or complementary treatments need to be developed. Melatonin exerts numerous physiological effects, including inducing anti‑inflammatory and antioxidative functions, resetting circadian rhythms and promoting wound healing and tissue regeneration. Melatonin also participates in the health management of bone and cartilage. In the present review, the potential roles of melatonin in the pathogenesis and progression of bone injury, osteoporosis, OA and periodontitis are summarized. Furthermore, the high efficiency and diversity of the physiological regulatory effects of melatonin are highlighted and the potential benefits of the use of melatonin for the clinical prevention and treatment of bone‑related diseases are discussed.
Keywords: melatonin; bone injury; osteoporosis; osteoarthritis; periodontitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
