

Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study
- PMID: 33760821
- PMCID: PMC7990210
- DOI: 10.1371/journal.pone.0241875
Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study
Abstract
Background: Prior studies examining symptoms of COVID-19 are primarily descriptive and measured among hospitalized individuals. Understanding symptoms of SARS-CoV-2 infection in pre-clinical, community-based populations may improve clinical screening, particularly during flu season. We sought to identify key symptoms and symptom combinations in a community-based population using robust methods.
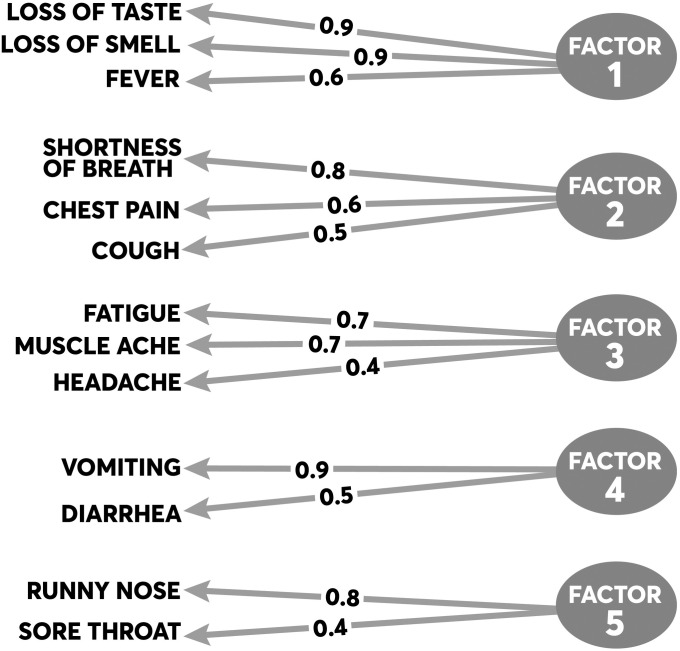
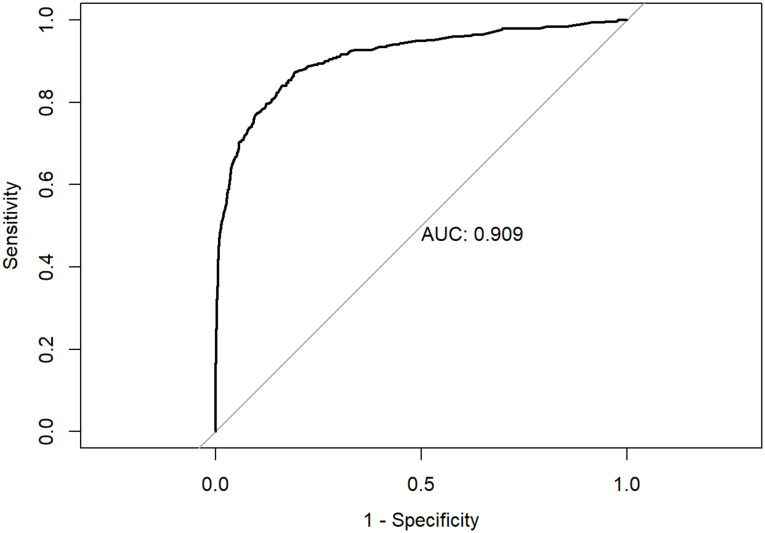
Methods: We pooled community-based cohorts of individuals aged 12 and older screened for SARS-CoV-2 infection in April and June 2020 for a statewide prevalence study. Main outcome was SARS-CoV-2 positivity. We calculated sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for individual symptoms as well as symptom combinations. We further employed multivariable logistic regression and exploratory factor analysis (EFA) to examine symptoms and combinations associated with SARS-CoV-2 infection.
Results: Among 8214 individuals screened, 368 individuals (4.5%) were RT-PCR positive for SARS-CoV-2. Although two-thirds of symptoms were highly specific (>90.0%), most symptoms individually possessed a PPV <50.0%. The individual symptoms most greatly associated with SARS-CoV-2 positivity were fever (OR = 5.34, p<0.001), anosmia (OR = 4.08, p<0.001), ageusia (OR = 2.38, p = 0.006), and cough (OR = 2.86, p<0.001). Results from EFA identified two primary symptom clusters most associated with SARS-CoV-2 infection: (1) ageusia, anosmia, and fever; and (2) shortness of breath, cough, and chest pain. Moreover, being non-white (13.6% vs. 2.3%, p<0.001), Hispanic (27.9% vs. 2.5%, p<0.001), or living in an Urban area (5.4% vs. 3.8%, p<0.001) was associated with infection.
Conclusions: Symptoms can help distinguish SARS-CoV-2 infection from other respiratory viruses, especially in community or urgent care settings where rapid testing may be limited. Symptoms should further be structured in clinical documentation to support identification of new cases and mitigation of disease spread by public health. These symptoms, derived from asymptomatic as well as mildly infected individuals, can also inform vaccine and therapeutic clinical trials.
Conflict of interest statement
No authors have competing interests.
Figures
Update of
-
Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study.medRxiv [Preprint]. 2020 Oct 22:2020.10.11.20210922. doi: 10.1101/2020.10.11.20210922. medRxiv. 2020. Update in: PLoS One. 2021 Mar 24;16(3):e0241875. doi: 10.1371/journal.pone.0241875. PMID: 33106813 Free PMC article. Updated. Preprint.
References
-
- Centers for Disease Control and Prevention US. Symptoms of Coronavirus Atlanta: CDC; 2020 [cited 2020 May 5]. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
-
- Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q, et al.. Prevalence of comorbidities and its effects in coronavirus disease 2019 patients: A systematic review and meta-analysis. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases. 2020;94:91–5. Epub 2020/03/17. 10.1016/j.ijid.2020.03.017 . - DOI - PMC - PubMed
-
- Struyf T, Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Leeflang MM, et al.. Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19 disease. The Cochrane database of systematic reviews. 2020;7(7):CD013665–CD. 10.1002/14651858.CD013665 . - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
