

Comparison of endoscopic ultrasound-guided choledochoduodenostomy and endoscopic retrograde cholangiopancreatography in first-line biliary drainage for malignant distal bile duct obstruction: A multicenter randomized controlled trial
- PMID: 33761729
- PMCID: PMC9282038
- DOI: 10.1097/MD.0000000000025268
Comparison of endoscopic ultrasound-guided choledochoduodenostomy and endoscopic retrograde cholangiopancreatography in first-line biliary drainage for malignant distal bile duct obstruction: A multicenter randomized controlled trial
Abstract
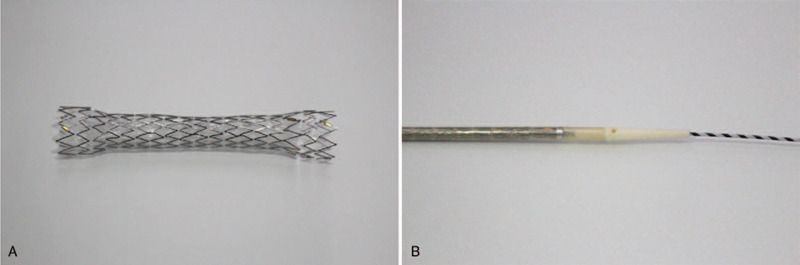
Introduction: In patients with malignant distal bile duct obstruction and normal gastrointestinal anatomy, endoscopic ultrasound-guided choledochoduodenostomy (EUS-CDS) is indicated when endoscopic retrograde cholangiopancreatography (ERCP) fails. The ERCP drainage route passes through the tumor, whereas the EUS-CDS route does not. Therefore, EUS-CDS is expected to have a longer stent patency than ERCP. However, for first-line biliary drainage, it remains unclear whether EUS-CDS or ERCP is superior in terms of stent patency. To reduce the frequency of highly adverse events (AEs) such as bile peritonitis or stent migration following EUS-CDS, we developed an antimigration metal stent with a thin delivery system for tract dilatation. This study is designed to assess whether EUS-CDS with this novel stent is superior to ERCP with a traditional metal stent in terms of stent patency when the two techniques are used for first-line drainage of malignant distal biliary obstruction.
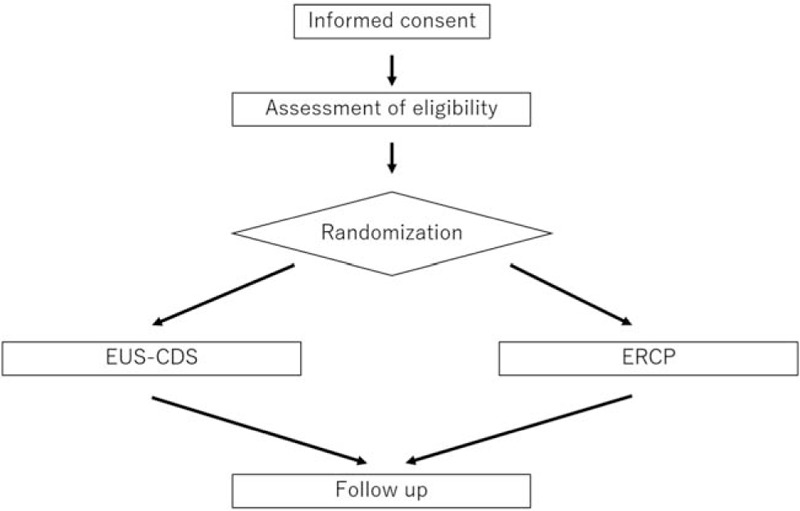
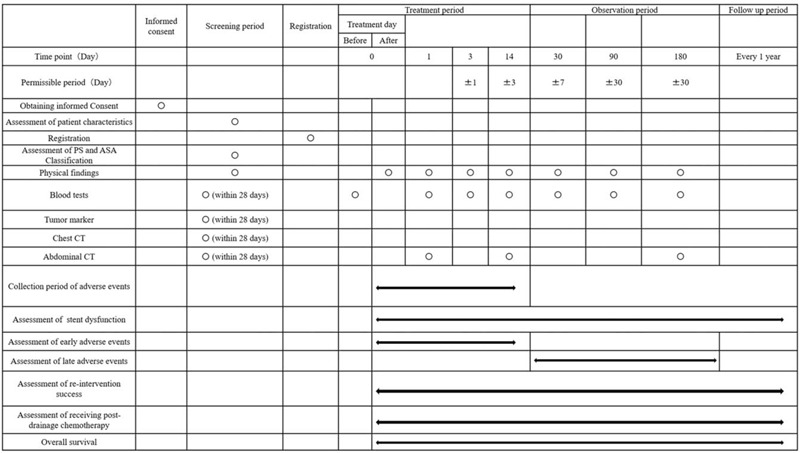
Methods/design: This study is a multicenter single-blinded randomized controlled trial (RCT) involving 95 patients in four tertiary centers. Patients with malignant distal biliary obstruction that is unresectable or presents a very high surgical risk and who pass the inclusion and exclusion criteria will be randomized to EUS-CDS or ERCP in a 1:1 proportion. The primary endpoint is the stent patency rate 180 days after stent insertion. Secondary outcomes include the rates of technical success, clinical success, technical success in cases not requiring fistulous-tract dilation (only EUS-CDS group), procedure-related AEs, re-intervention success, patients receiving post-drainage chemotherapy, procedure time, and overall survival time.
Discussion: If EUS-CDS is superior to ERCP in terms of stent patency and safety for the first-line drainage of malignant distal biliary obstruction, it is expected that the first-line drainage method will be changed from ERCP to EUS-CDS, and that interruption of chemotherapy due to stent dysfunction can be avoided.
Trial registration: University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR), ID: UMIN000041343. Registered on August 6, 2020. https://upload.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000047201Version number: 1.2, December 7, 2020.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
Endoscopic Ultrasound-Guided Biliary Drainage of First Intent With a Lumen-Apposing Metal Stent vs Endoscopic Retrograde Cholangiopancreatography in Malignant Distal Biliary Obstruction: A Multicenter Randomized Controlled Study (ELEMENT Trial).Gastroenterology. 2023 Nov;165(5):1249-1261.e5. doi: 10.1053/j.gastro.2023.07.024. Epub 2023 Aug 6. Gastroenterology. 2023. PMID: 37549753 Clinical Trial.
-
ELEMENT TRIAL: study protocol for a randomized controlled trial on endoscopic ultrasound-guided biliary drainage of first intent with a lumen-apposing metal stent vs. endoscopic retrograde cholangio-pancreatography in the management of malignant distal biliary obstruction.Trials. 2019 Dec 9;20(1):696. doi: 10.1186/s13063-019-3918-y. Trials. 2019. PMID: 31818329 Free PMC article.
-
Endoscopic ultrasound-guided choledochoduodenostomy using a thin stent delivery system in patients with unresectable malignant distal biliary obstruction: A prospective multicenter study.Dig Endosc. 2019 May;31(3):291-298. doi: 10.1111/den.13300. Epub 2018 Dec 18. Dig Endosc. 2019. PMID: 30444543
-
Primary drainage of distal malignant biliary obstruction: A comparative network meta-analysis.Dig Liver Dis. 2024 Dec;56(12):2004-2010. doi: 10.1016/j.dld.2024.08.053. Epub 2024 Sep 13. Dig Liver Dis. 2024. PMID: 39277511
-
Combination of endoscopic retrograde cholangiopancreatography and endoscopic ultrasonography-guided biliary drainage in malignant hilar biliary obstruction.Dig Endosc. 2019 Apr;31 Suppl 1:50-54. doi: 10.1111/den.13371. Dig Endosc. 2019. PMID: 30994233 Review.
Cited by
-
Treatment of obstructive jaundice induced by non-hodgkin lymphoma with EUS-guided transgastric anterograde common bile duct stenting: Technical case report and literature review.Front Surg. 2023 Jan 6;9:1031718. doi: 10.3389/fsurg.2022.1031718. eCollection 2022. Front Surg. 2023. PMID: 36684212 Free PMC article.
-
Endoscopy Ultrasound-Guided Biliary Drainage Using Lumen Apposing Metal Stent in Malignant Biliary Obstruction.Diagnostics (Basel). 2023 Aug 29;13(17):2788. doi: 10.3390/diagnostics13172788. Diagnostics (Basel). 2023. PMID: 37685326 Free PMC article. Review.
-
Current landscape of therapeutic EUS: Changing paradigms in gastroenterology practice.Endosc Ultrasound. 2023 Jan-Feb;12(1):16-28. doi: 10.4103/EUS-D-21-00177. Endosc Ultrasound. 2023. PMID: 36124531 Free PMC article. Review.
-
Multicenter study of lumen-apposing metal stents with or without pigtail in endoscopic ultrasound-guided biliary drainage for malignant obstruction-BAMPI TRIAL: an open-label, randomized controlled trial protocol.Trials. 2022 Feb 25;23(1):181. doi: 10.1186/s13063-022-06106-1. Trials. 2022. PMID: 35216619 Free PMC article.
-
Biliary drainage in malignant biliary obstruction: an umbrella review of randomized controlled trials.Front Oncol. 2023 Sep 5;13:1235490. doi: 10.3389/fonc.2023.1235490. eCollection 2023. Front Oncol. 2023. PMID: 37731638 Free PMC article. Review.
References
-
- Das A, Sivak MV, jr. Endoscopic palliation for inoperable pancreatic cancer. Cancer Control 2000;7:452–7. - PubMed
-
- Inamdar S, Slattery E, Bhalla R, et al. Comparison of adverse events for endoscopic vs percutaneous biliary drainage in the treatment of malignant biliary tract obstruction in an inpatient national cohort. JAMA Oncol 2016;2:112–7. - PubMed
-
- Almadi MA, Barkun A, Martel M. Plastic vs. self-expandable metal stents for palliation in malignant biliary obstruction: a series of meta-analyses. Am J Gastroenterol 2017;112:260–73. - PubMed
-
- Minaga K, Kitano M. Recent advances in endoscopic ultrasound-guided biliary drainage. Dig Endosc 2018;30:38–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
