

All-arthroscopic repair of Atzei class II and III triangular fibrocartilage complex tears using the FasT-Fix suture device
- PMID: 33761973
- PMCID: PMC7989095
- DOI: 10.1186/s13018-020-02046-1
All-arthroscopic repair of Atzei class II and III triangular fibrocartilage complex tears using the FasT-Fix suture device
Abstract
Background: The study is aimed to propose an arthroscopic repair technique using a pre-tied suture device for peripheral TFCC (triangular fibrocartilage complex) tear with proximal component involvement.
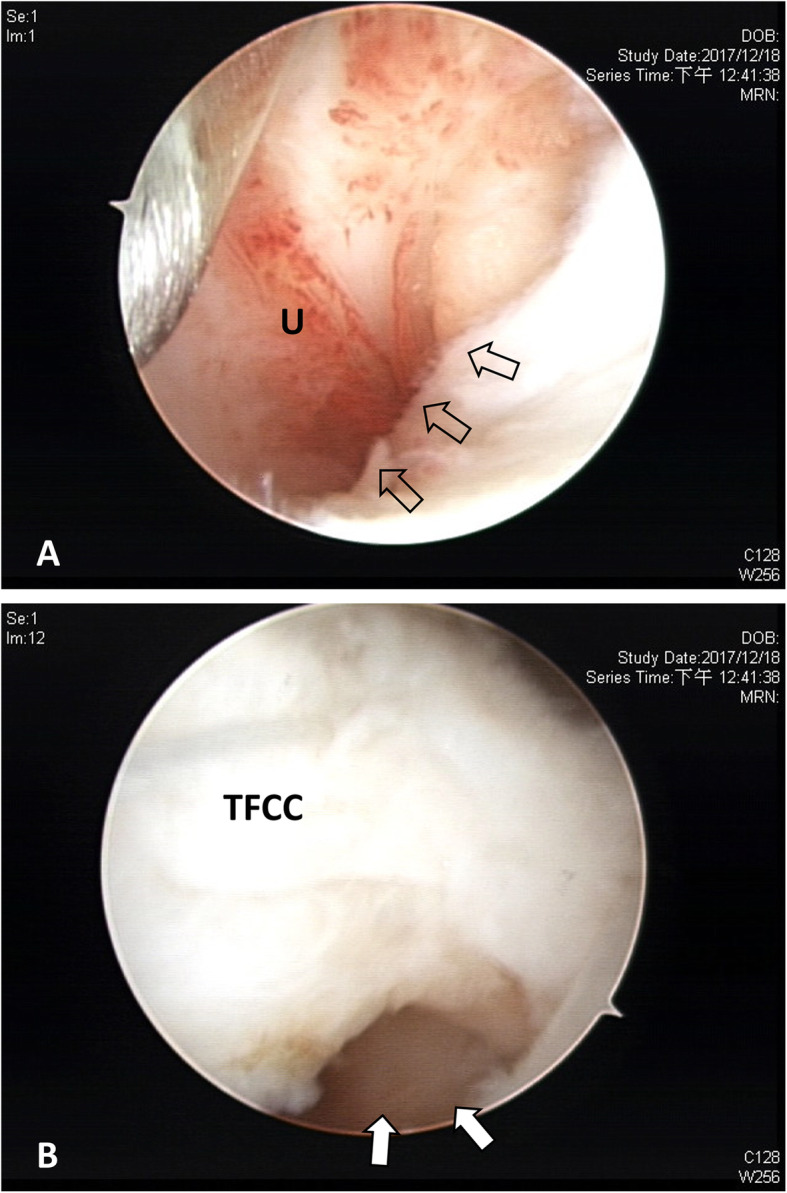
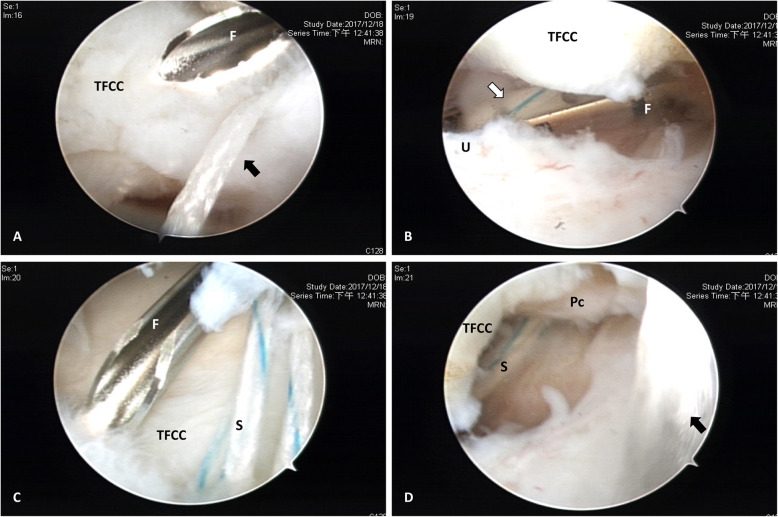
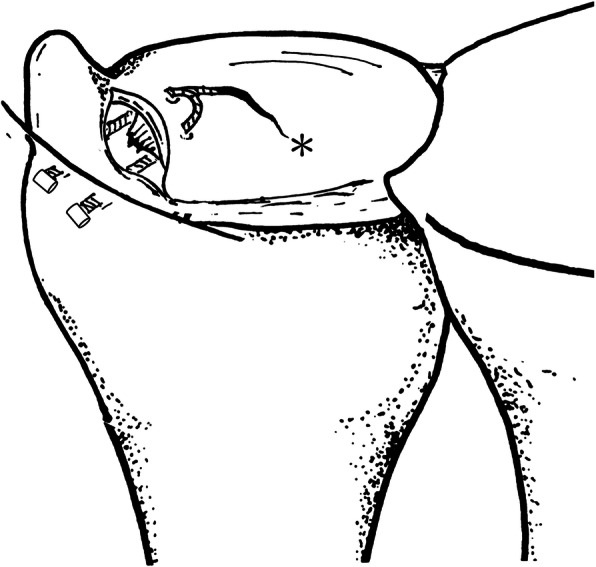
Methods: Through a retrospective review in the medical records of patients who underwent unilateral arthroscopic repair for TFCC Palmer IB lesion between 2017 and 2019, 12 patients were arthroscopically diagnosed as proximal component tear and received more than 1 year follow-up postoperatively. The arthroscope was introduced from 6R portal to discriminate Atzei class II from III lesions by a "visualization test" and to supervise the repair procedure using pre-tied FasT-Fix suture device from 3-4 portal. Two poly-ether-ether-ketone (PEEK) blocks were further advanced along the device needle to finally seat outside the ulnar joint capsule, followed by gradually tightening the pre-tied suture loop until the TFCC periphery was securely repositioned and held stably.
Results: Operation time averaged 87 min. Hook test and DRUJ arthroscopy confirmed proximal component tear in all 12 wrists. Four patients were diagnosed to be Atzei class II lesion as full thickness tear of distal component was arthroscopically identified from 6R portal while the other 8 exhibited partial thickness tear and were categorized as class III lesion. Follow-up averaged 15 months with a range of 12 to 24 months. Mayo modified wrist score improved from an average of 61.3 preoperatively to 90.4 at the latest visit.
Conclusions: A modified technique for diagnosis and all-arthroscopic repair in TFCC Atzei class II and III lesions using a pre-tied suture device is a feasible and safe option with promising results.
Keywords: Arthroscopy; Distal radioulnar joint; Peripheral tear; Triangular fibrocartilage complex.
Conflict of interest statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. The authors report no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
