

Bone mineral density changes in a free vascularised fibular graft in the distal femoral bone after osteosarcoma in a 10-year-old boy: a 7-year follow-up
- PMID: 33762269
- PMCID: PMC7993341
- DOI: 10.1136/bcr-2020-236097
Bone mineral density changes in a free vascularised fibular graft in the distal femoral bone after osteosarcoma in a 10-year-old boy: a 7-year follow-up
Abstract
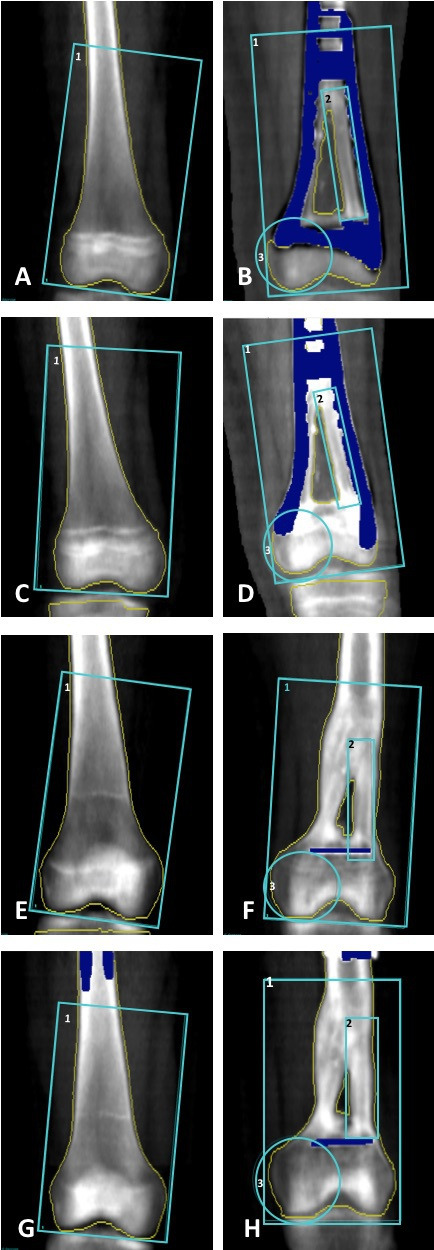
A 10-year-old boy presented with continuous reports of pain located to the left knee. Imaging revealed a sclerotic process in the left distal femur, and biopsies were consistent with chondroblastic osteosarcoma. As part of standard treatment the patient underwent neoadjuvant chemotherapy followed by limb sparring surgery and adjuvant chemotherapy. The entire tumour was excised and femoral bone reconstruction was performed with a double barrel free vascularised fibular graft. Bone mineral density (BMD) can be decreased in childhood survivors of cancer. The patient was followed for 7 years with dual-energy X-ray absorptiometry scans in order to assess BMD and graft adaption. Despite two accidental fractures to the graft region local and global BMD underwent an overall increase. Approximately 7 years after tumour resection the patient had a global Z-score of 0.2, which is considered within normal range.
Keywords: cancer intervention; orthopaedics; osteoporosis; paediatric oncology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures









References
-
- Bacci G, Ferrari S, Bertoni F, et al. . Long-Term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Istituto ortopedico rizzoli according to the Istituto ortopedico rizzoli/osteosarcoma-2 protocol: an updated report. J Clin Oncol 2000;18:4016–27. 10.1200/JCO.2000.18.24.4016 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials