

Dynamics of cerebral perfusion and oxygenation parameters following endovascular treatment of acute ischemic stroke
- PMID: 33762405
- PMCID: PMC8785045
- DOI: 10.1136/neurintsurg-2020-017163
Dynamics of cerebral perfusion and oxygenation parameters following endovascular treatment of acute ischemic stroke
Abstract
Background: We studied the effects of endovascular treatment (EVT) and the impact of the extent of recanalization on cerebral perfusion and oxygenation parameters in patients with acute ischemic stroke (AIS) and large vessel occlusion (LVO).
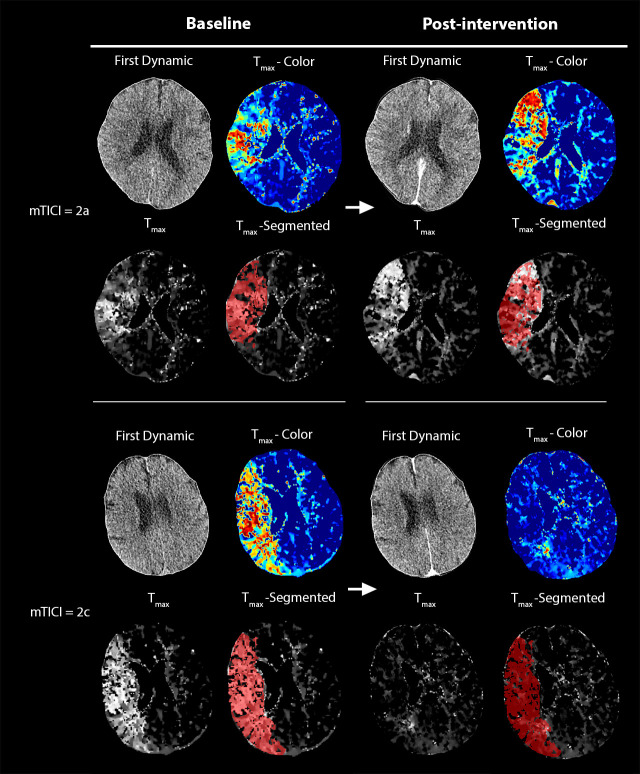
Methods: Forty-seven patients with anterior LVO underwent computed tomography perfusion (CTP) before and immediately after EVT. The entire ischemic region (Tmax >6 s) was segmented before intervention, and tissue perfusion (time-to-maximum (Tmax), time-to-peak (TTP), mean transit time (MTT), cerebral blood volume (CBV), cerebral blood flow (CBF)) and oxygenation (coefficient of variation (COV), capillary transit time heterogeneity (CTH), metabolic rate of oxygen (CMRO2), oxygen extraction fraction (OEF)) parameters were quantified from the segmented area at baseline and the corresponding area immediately after intervention, as well as within the ischemic core and penumbra. The impact of the extent of recanalization (modified Treatment in Cerebral Infarction (mTICI)) on CTP parameters was assessed with the Wilcoxon test and Pearson's correlation coefficients.
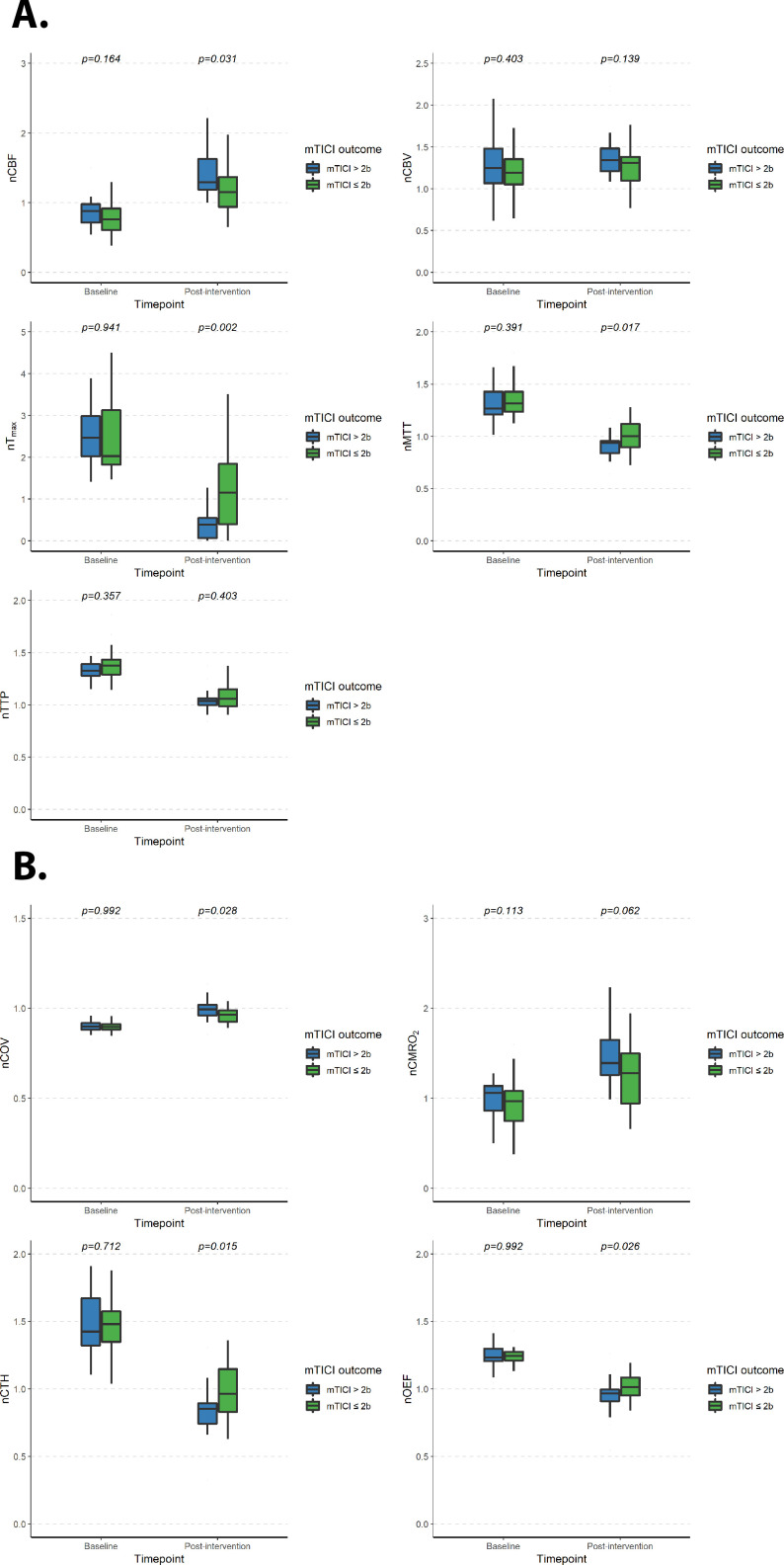
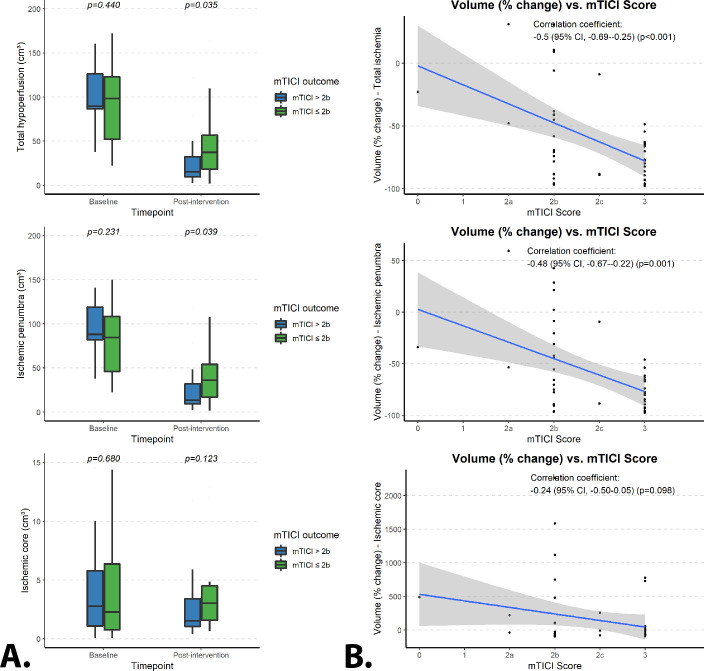
Results: The Tmax, MTT, OEF and CTH values immediately after EVT were lower in patients with complete (as compared with incomplete) recanalization, whereas CBF and COV values were higher (P<0.05) and no differences were found in other parameters. The ischemic penumbra immediately after EVT was lower in patients with complete recanalization as compared with those with incomplete recanalization (P=0.002), whereas no difference was found for the ischemic core (P=0.12). Specifically, higher mTICI scores were associated with a greater reduction of ischemic penumbra volumes (R²=-0.48 (95% CI -0.67 to -0.22), P=0.001) but not of ischemic core volumes (P=0.098).
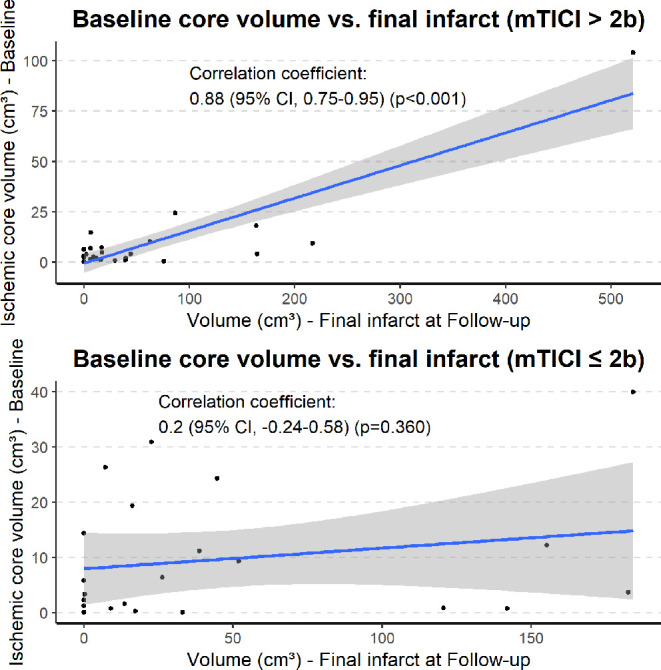
Conclusions: Our study demonstrates that the ischemic penumbra is the key target of successful EVT in patients with AIS and largely determines its efficacy on a tissue level. Furthermore, we confirm the validity of the mTICI score as a surrogate parameter of interventional success on a tissue perfusion level.
Keywords: CT perfusion; angiography; intervention; stroke; thrombectomy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Additionally, the authors disclose the following relationships with companies unrelated to this research project. SN: consultancy: Brainomix, Boehringer Ingelheim; payment for lectures including service on speakers' bureaus: Pfizer, Medtronic, Bayer AG. CH: consultancy: Brainomix, Oxford, UK; comments: <€10,000. CU: travel/accommodation/meeting expenses unrelated to activities listed: MicroVention, Stryker. SH: grants/grants pending: Deutsche Forschungsgemeinschaft (DFG) - SFB 1118. MB: board membership: Data and Safety Monitoring Board for Vascular Dynamics, Guerbet, Boehringer Ingelheim; consultancy: Codman, Roche Diagnostics, Guerbet, Boehringer Ingelheim, BBRaun, Merck; grants/grants pending: DFG, Hopp Foundation, Novartis, Siemens, Guerbet, Stryker, Covidien, EU; payment for lectures including service on speakers' bureaus: Novartis, Roche Diagnostics, Guerbet, Teva Pharmaceutical Industries, Bayer AG, Codman. MM: board membership: Codman; consultancy: Medtronic, MicroVention, Stryker; payment for lectures including service on speakers' bureaus: Medtronic, MicroVention, Stryker; grants/grants pending: Balt. *Money paid to the institution. JARP: payment for lectures including service on speakers' bureaus: Siemens; travel/accommodation/meeting expenses unrelated to activities listed: Stryker, MicroVention. PAR: consultancy: Bayer, Pfizer, Daiichi Sankyo; personal fees: Boehringer Ingelheim.
Figures
References
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019;50:e344–418. 10.1161/STR.0000000000000211 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical