

Repurposed drugs block toxin-driven platelet clearance by the hepatic Ashwell-Morell receptor to clear Staphylococcus aureus bacteremia
- PMID: 33762439
- PMCID: PMC9121309
- DOI: 10.1126/scitranslmed.abd6737
Repurposed drugs block toxin-driven platelet clearance by the hepatic Ashwell-Morell receptor to clear Staphylococcus aureus bacteremia
Abstract
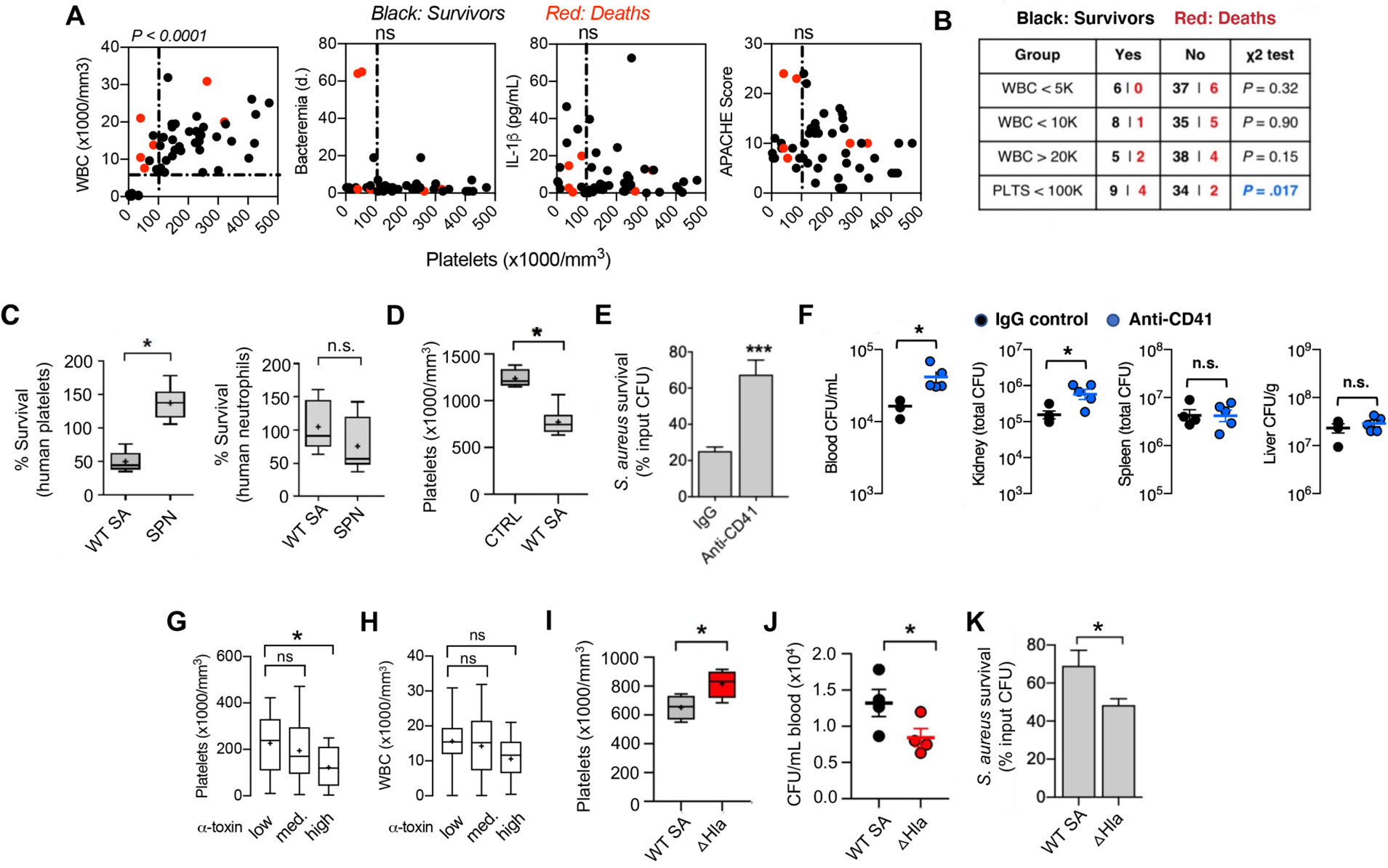
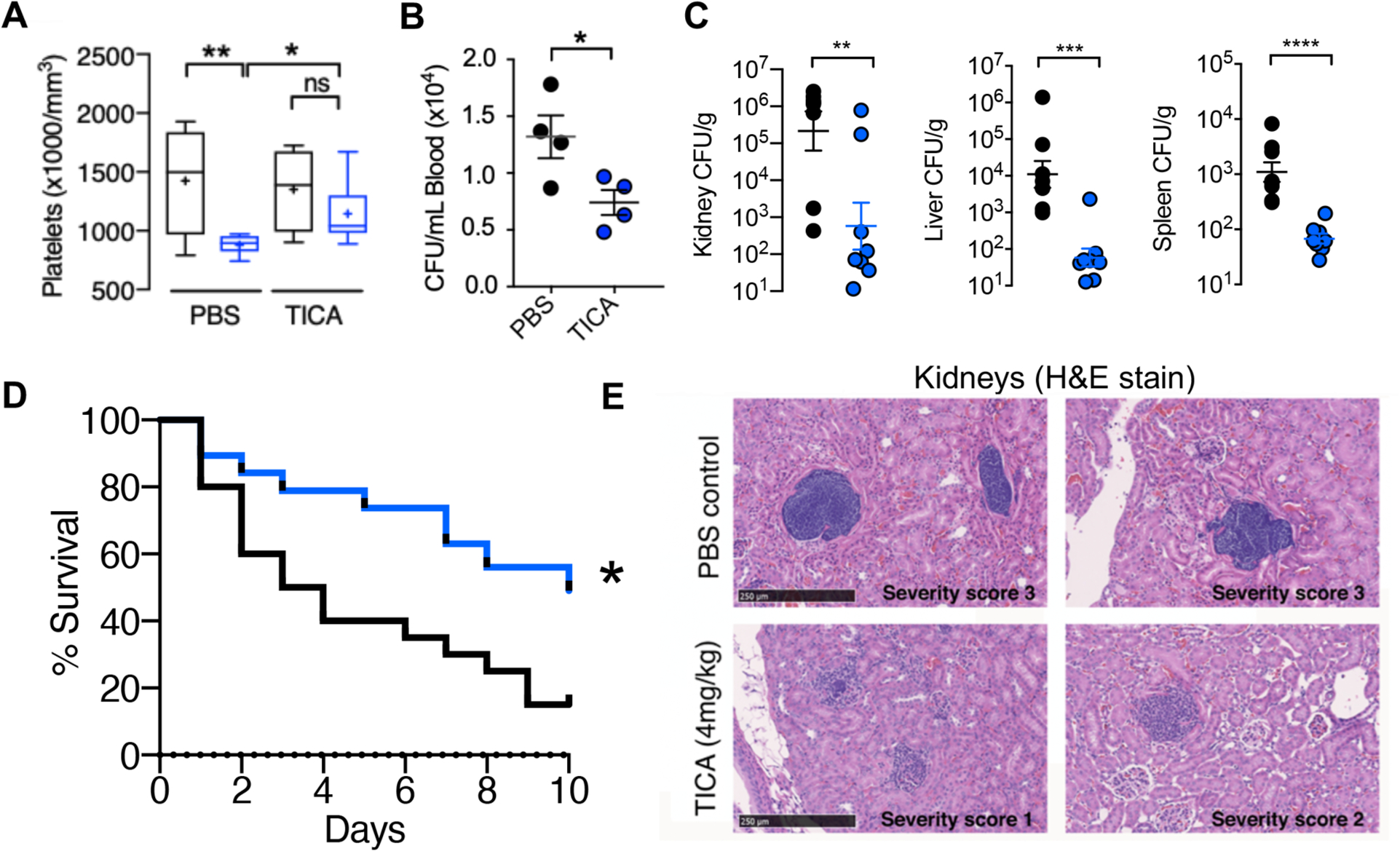
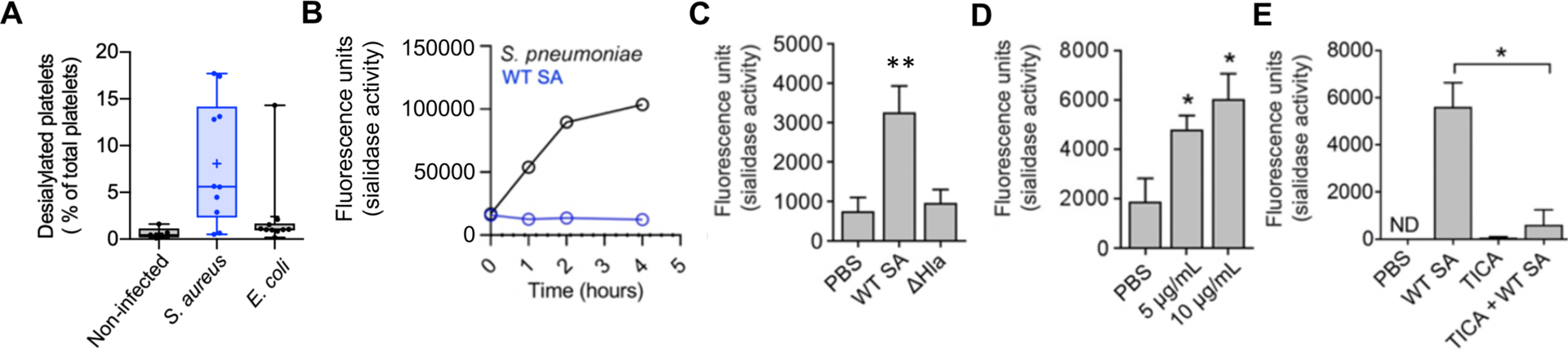
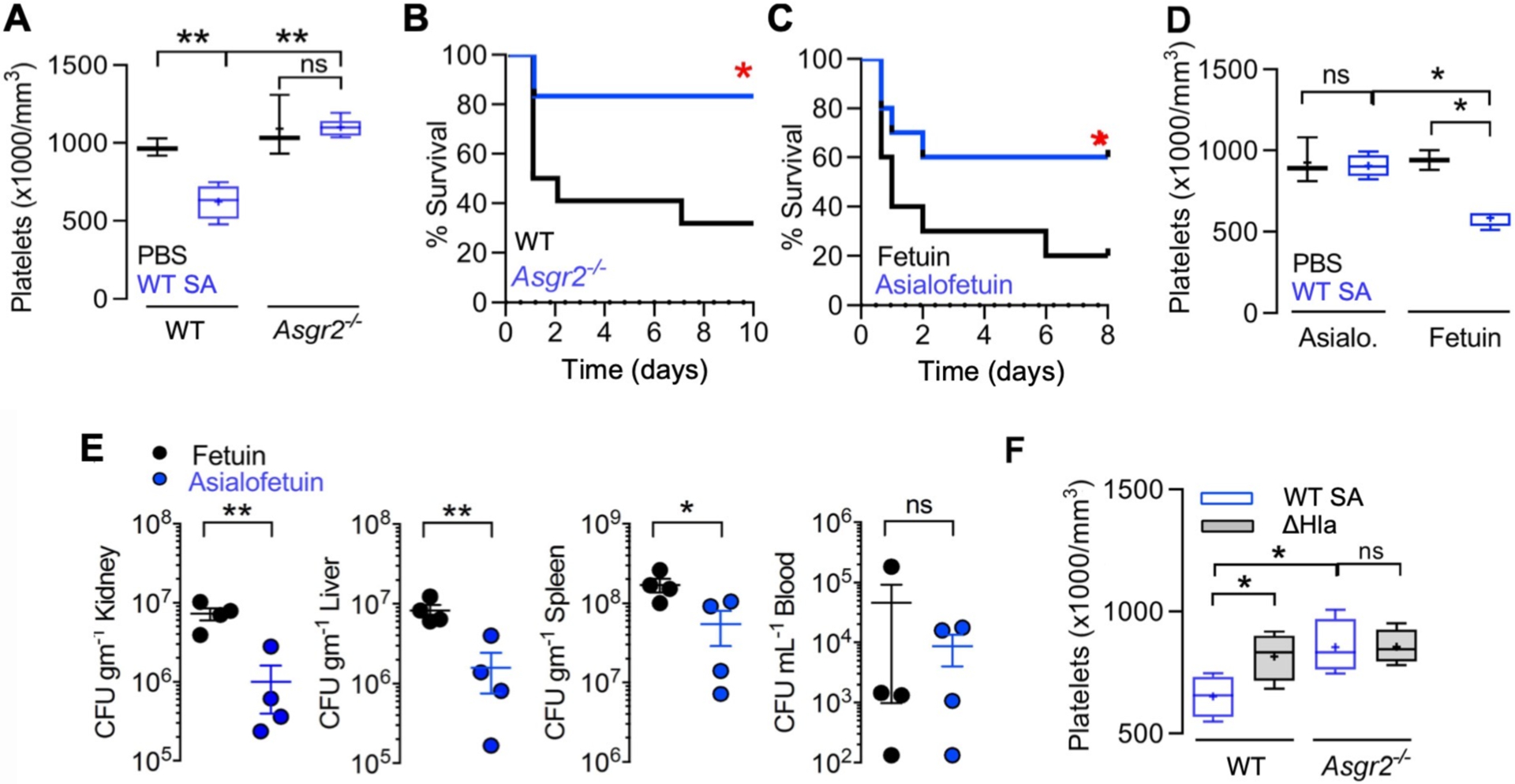
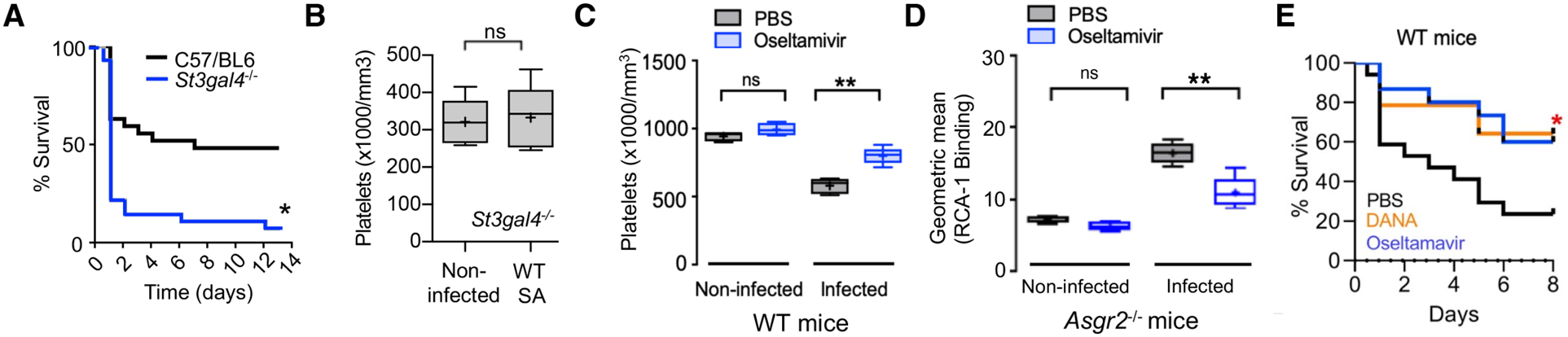
Staphylococcus aureus (SA) bloodstream infections cause high morbidity and mortality (20 to 30%) despite modern supportive care. In a human bacteremia cohort, we found that development of thrombocytopenia was correlated to increased mortality and increased α-toxin expression by the pathogen. Platelet-derived antibacterial peptides are important in bloodstream defense against SA, but α-toxin decreased platelet viability, induced platelet sialidase to cause desialylation of platelet glycoproteins, and accelerated platelet clearance by the hepatic Ashwell-Morell receptor (AMR). Ticagrelor (Brilinta), a commonly prescribed P2Y12 receptor inhibitor used after myocardial infarction, blocked α-toxin-mediated platelet injury and resulting thrombocytopenia, thereby providing protection from lethal SA infection in a murine intravenous challenge model. Genetic deletion or pharmacological inhibition of AMR stabilized platelet counts and enhanced resistance to SA infection, and the anti-influenza sialidase inhibitor oseltamivir (Tamiflu) provided similar therapeutic benefit. Thus, a "toxin-platelet-AMR" regulatory pathway plays a critical role in the pathogenesis of SA bloodstream infection, and its elucidation provides proof of concept for repurposing two commonly prescribed drugs as adjunctive therapies to improve patient outcomes.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures

References
-
- Laupland KB, Incidence of bloodstream infection: a review of population-based studies, Clin. Microbiol. Infect 19, 492–500 (2013). - PubMed
-
- Kaasch AJ, Barlow G, Edgeworth JD, Fowler VG Jr, Hellmich M, Hopkins S, Kern WV, Llewelyn MJ, Rieg S, Rodriguez-Baño J, Scarborough M, Seifert H, Soriano A, Tilley R, Tőrők ME, Weiß V, Wilson APR, Thwaites GE, ISAC, INSTINCT, SABG, UKCIRG, and Colleagues, Staphylococcus aureus bloodstream infection: a pooled analysis of five prospective, observational studies, J. Infect 68, 242–251 (2014). - PMC - PubMed
-
- Del Rio A, Cervera C, Moreno A, Patients at risk of complications of Staphylococcus aureus bloodstream infection, Clin. Infect. Dis 48 Suppl 4:S246–53 (2009) - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
