

Added value of computed tomography fractional flow reserve in the diagnosis of coronary artery disease
- PMID: 33762686
- PMCID: PMC7991632
- DOI: 10.1038/s41598-021-86245-8
Added value of computed tomography fractional flow reserve in the diagnosis of coronary artery disease
Abstract
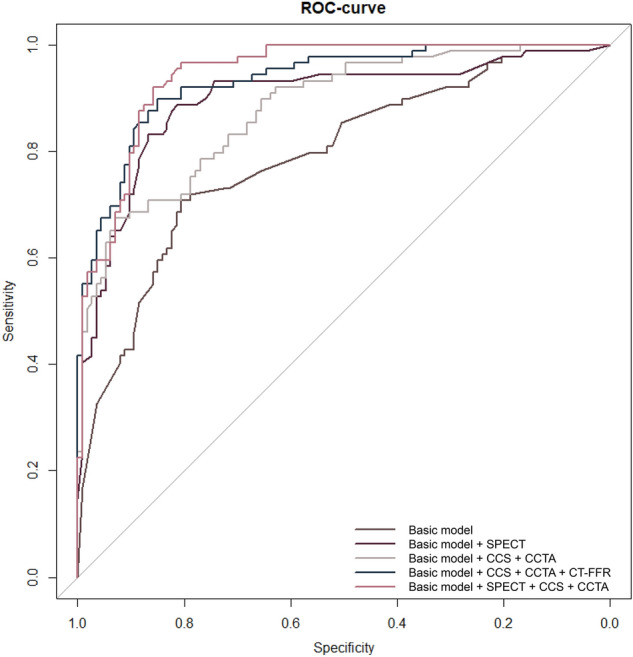
Multiple non-invasive tests are performed to diagnose coronary artery disease (CAD), but all are limited to either anatomical or functional assessments. Computed tomography derived Fractional Flow Reserve (CT-FFR) based on patient-specific lumped parameter models is a new test combining both characteristics simulating invasive FFR. This study aims to evaluate the added value of CT-FFR over other non-invasive tests to diagnose CAD. Patients with clinical suspicion of angina pectoris between 2010 and 2011 were included in this cross-sectional study. All underwent stress electrocardiography (X-ECG), SPECT, CT coronary angiography (CCTA) and CT-FFR. Invasive coronary angiography (ICA) and FFR were used as reference standard. Five models mimicking the clinical workflow were fitted and the area under receiver operating characteristic (AUROC) curve was used for comparison. 44% of the patients included in the analysis had a FFR of ≤ 0.80. The basic model including pre-test-likelihood and X-ECG had an AUROC of 0.79. The SPECT-strategy had an AUROC of 0.90 (p = 0.008), CCTA-strategy of 0.88 (p < 0.001), 0.93 when adding CT-FFR (p = 0.40) compared to 0.94 when combining CCTA and SPECT. This study shows adding on-site CT-FFR based on patient-specific lumped parameter models leads to an increased AUROC compared to the basic model. It improves the diagnostic work-up beyond SPECT or CCTA and is non-inferior to the combined strategy of SPECT and CCTA in the diagnosis of hemodynamically relevant CAD.
Conflict of interest statement
Dr. M.J. Swaans reports personal fees from consultancy for Abbott Vascular, Boston Scientific, Philips Healthcare and Bioventrix Inc., outside the submitted work. Prof. Dr. T. Leiner received grants from the Dutch Technology Foundation (P15-26, 12726), with participation of Pie Medical Imaging and Philips Healthcare, from the Netherlands Organisation for Health Research and Development, with participation of Pie Medical Imaging, and from Pie Medical Imaging; holds stock in Quantib-U; is cofounder, scientific lead, and a shareholder at Quantib-U. The other authors declare no competing interests.
Figures


References
-
- Task Force Members. Montalescot G, Sechtem U, Achenbach S, Andreotti F, Arden C, Budaj A, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur. Heart J. 2013;34:2949–3003. doi: 10.1093/eurheartj/eht296. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
