

Screen Fast, Screen Faster: A Pilot Study to Screen for Depressive Symptoms Using the Beck Depression Inventory Fast Screen in Parkinson's Disease With Mild Cognitive Impairment
- PMID: 33763020
- PMCID: PMC7982682
- DOI: 10.3389/fneur.2021.640137
Screen Fast, Screen Faster: A Pilot Study to Screen for Depressive Symptoms Using the Beck Depression Inventory Fast Screen in Parkinson's Disease With Mild Cognitive Impairment
Abstract
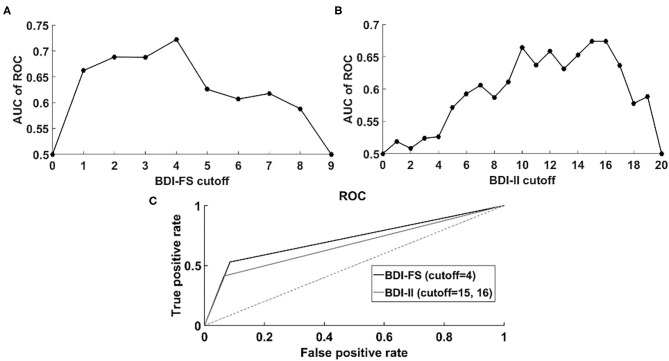
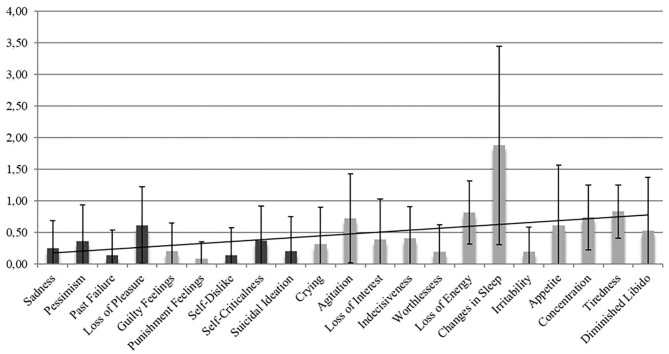
Objective: Depressive symptoms have a high prevalence in patients with Parkinson's disease (PD) and are associated with cognitive dysfunction. Especially in PD with mild cognitive impairment (MCI), a time-efficient and valid instrument for the assessment of depression primarily focusing on psychological symptoms and disregarding confounding somatic symptoms is needed. We performed an examination of the psychometric properties of the Beck Depression Inventory II (BDI-II) and the Beck Depression Inventory Fast Screen (BDI-FS). Methods: The sample consisted of 64 patients [22 females and 42 males, mean age: 67.27 years (SD = 7.32)]. Depressive symptoms were measured in a cohort of PD patients with MCI. For the BDI-II and BDI-FS the psychometric concepts of internal consistency, convergent validity and diagnostic agreement were assessed. Results: Patients gave higher ratings on test items addressing somatic symptoms than those addressing non-somatic ones. The correlation between the absolute total scores of the BDI-II and the BDI-FS was significant (r = 0.91, p < 0.001), which indicated convergent validity. The Cronbach's alpha values indicated adequate internal consistencies for both measures (BDI-II: 0.84; BDI-FS: 0.78). There was a higher than chance level agreement of diagnoses of the two questionnaires, measured by Cohen's kappa (0.58, p < 0.001). The agreements between previous diagnosis of depression and the diagnoses of the BDI-II/BDI-FS were also significantly higher than chance level (BDI-II: 0.34, p = 0.007, BDI-FS: 0.39, p = 0.002). Additional AUC analysis across different cutoffs showed that performance of BDI-FS was better than BDI-II, supporting the observation of an equivalent or better performance of BDI-FS than BDI-II. Importantly, AUC analysis confirmed that a cutoff = 4 for BDI-FS was suitable in the considered sample of patients with PD-MCI. Discussion: In a cohort of PD-MCI, the BDI-FS demonstrates adequate psychometric properties in comparison to the BDI-II and can be used as a screening measure for assessing depression in cognitively impaired PD patients, focusing solely on psychological symptoms. Still, further research is needed to validate this instrument.
Keywords: BDI-FS; BDI-II; Parkinson's disease; depression; mild cognitive impairment.
Copyright © 2021 Elben, Dimenshteyn, Trenado, Folkerts, Ophey, Sulzer, Becker, Schmidt, Tödt, Witt, Liepelt-Scarfone, Yilmaz, Kalbe and Wojtecki.
Conflict of interest statement
AK-F has received a grant from the German Parkinson Society and honoraria from ProLog Wissen GmbH, Cologne, Germany, and pro audito Switzerland, Zürich, Switzerland. NS has received grants from the German Federal Ministry of Education and Research. KW has received grants for the German Research Foundation, the German Federal Ministry of Education and Research, and received speaker honoraria from BIAL, BAYER, Medtronic, Boston Scientific, Novartis, Desitin, and the German Society of Neurology. IL-S has received grants from the Parkinson Fonds Deutschland gGmbH, Janssen Pharmaceutical Companies of Johnson & Johnson, European Commission, H2020-TWINN-2015, and the Michael J. Fox Foundation. EK has received grants from the German Ministry of Education and Research, Parkinson Fonds Deutschland gGmbH, and the German Parkinson Society and honoraria from Oticon GmbH, Hamburg, Germany; Lilly Pharma GmbH, Bad Homburg, Germany; Bernafon AG, Bern, Switzerland; and Desitin GmbH, Hamburg, Germany. LW has received honoraria from Meda, Boehringer, Cephalon Pharma, TEVA, Desitin, AbbVie St. Jude Medical / Abbott, and Medtronic and grants from HHU Düsseldorf, DFG Forschergruppe (FOR 1328), ERANET Neuron/BMBF (TYMON 01EW141), German Parkinson's Disease Association (dPV), Parkinson Fonds Germany, and Hilde Ulrichs Stiftung für Parkinsonforschung. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources