

Frailty impact on postoperative complications and early mortality rates in patients undergoing radical cystectomy for bladder cancer: a systematic review
- PMID: 33763244
- PMCID: PMC7954492
- DOI: 10.1080/2090598X.2020.1841538
Frailty impact on postoperative complications and early mortality rates in patients undergoing radical cystectomy for bladder cancer: a systematic review
Abstract
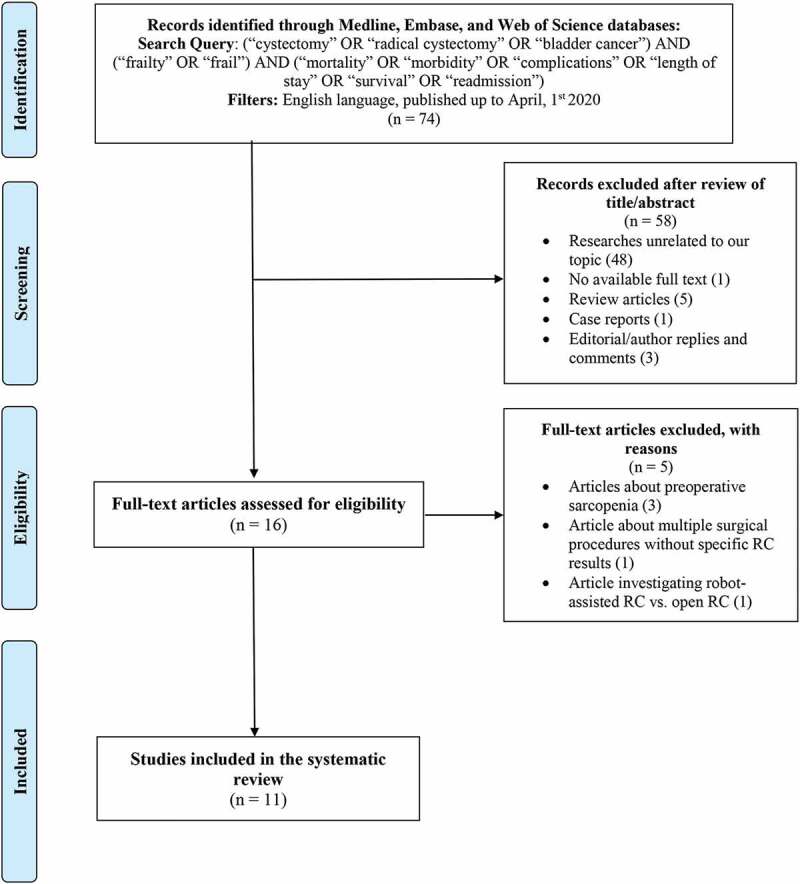
Objective: To assess the prevalence of frailty, a status of vulnerability to stressors leading to adverse health events, in bladder cancer patients undergoing radical cystectomy (RC), and test the impact of frailty measurements on postoperative adverse outcomes. Methods: A systematic review of English-language articles published up to April 2020 was performed. Electronic databases were searched to quantify the frailty prevalence in RC patients and assess the predictive ability of frailty indexes on RC-related outcomes as postoperative complications, early mortality, hospitalization length (LOS), costs, discharge dispositions, readmission rate. Results: Eleven studies were selected. Patients' frailty was identified by Johns Hopkins indicator (JHI) in two studies, 11-item modified Frailty Index (mFI) in four, 5-item simplified FI (sFI) in three, 15-point mFI in one, Fried Frailty Criteria in one. Considering all the frailty measurements applied, 8% and 31% of patients were frail or pre-frail, respectively. Frail (43%) and pre-frail patients (35%) were more at risk of major complications compared to non-frail (27%) using sFI; with JHI the percentages of frail and non-frail were 53% versus 19%. According to JHI and mFI frailty was related to longer LOS and higher costs. JHI identified that 3% of frail patients experience in-hospital mortality versus 1.5% of non-frail. Finally, using sFI, frail (28%), and pre-frail (19%) were more likely to be discharged non-home compared to non-frail patients (8%) and had a higher risk of 30-day mortality (4% and 2% versus 1%). Conclusions: Almost half of RC patients were frail or pre-frail, conditions significantly related to an increased risk of postoperative adverse events with higher rates of major complications and early mortality. The most-used frailty index was mFI, while JHI and sFI resulted the most reliable to predict early postoperative RC-related adverse outcomes and should be routinely included in clinical practice after better standardization throughout prospective comparative studies. Abbreviations: ACG: Adjusted Clinical Groups; ACS: American College Surgeons; AUC: area under the curve; BCa: bladder cancer; CCI: Charlson Comorbidity Index; CSHA-FI: Canadian Study of Health and Aging Frailty Index; CCS: Clavien-Dindo Classification Score; ERAS: Enhanced Recovery After Surgery; FFC: Fried Frailty Criteria; (e)(m)(s)FI: (extended) (modified) (simplified) Frailty Index; ICU: intensive care unit; IQR: interquartile range; (p)LOS: (prolonged) length of hospital stay; NSQIP: National Surgical Quality Improvement Program; OR: odds ratio; (O)PN: (open) partial nephrectomy; PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses; (O)(RA)RC: (open)(robot-assisted) radical cystectomy; (O)RN: (open) radical nephrectomy; ROC: receiver operating characteristic; RNU: radical nephroureterectomy; (R)RP: (retropubic) radical prostatectomy; RR: relative risk; THCs: total hospital charges; nephrectomy; UD: urinary diversion.
Keywords: Bladder cancer; complications; cystectomy; frailty; mortality.
© 2020 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group.
Conflict of interest statement
The authors certify that there is no conflict of interest with any financial organisation regarding the material discussed in the manuscript.
Figures
References
-
- Siegel RL, Miller KD, Jemal A.. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. - PubMed
-
- EAU Guidelines . Edn. presented at the EAU Annual congress amsterdam 2020. ISBN 978–94–92671–07–3. EAU Guidelines Office, Arnhem, The Netherlands. http://uroweb.org/guidelines/compilations-of-all-guidelines/
-
- Abufaraj M, Foerster B, Schernhammer E, et al. Micropapillary urothelial carcinoma of the bladder: a systematic review and meta-analysis of disease characteristics and treatment outcomes. Eur Urol. 2019;75(4):649–658. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous