

Noninvasive Assessment of Right Ventricle Function and Pulmonary Artery Pressure Using Transthoracic Echocardiography in Women With Pre-Eclampsia: An Exploratory Study
- PMID: 33763315
- PMCID: PMC7980723
- DOI: 10.7759/cureus.13419
Noninvasive Assessment of Right Ventricle Function and Pulmonary Artery Pressure Using Transthoracic Echocardiography in Women With Pre-Eclampsia: An Exploratory Study
Abstract
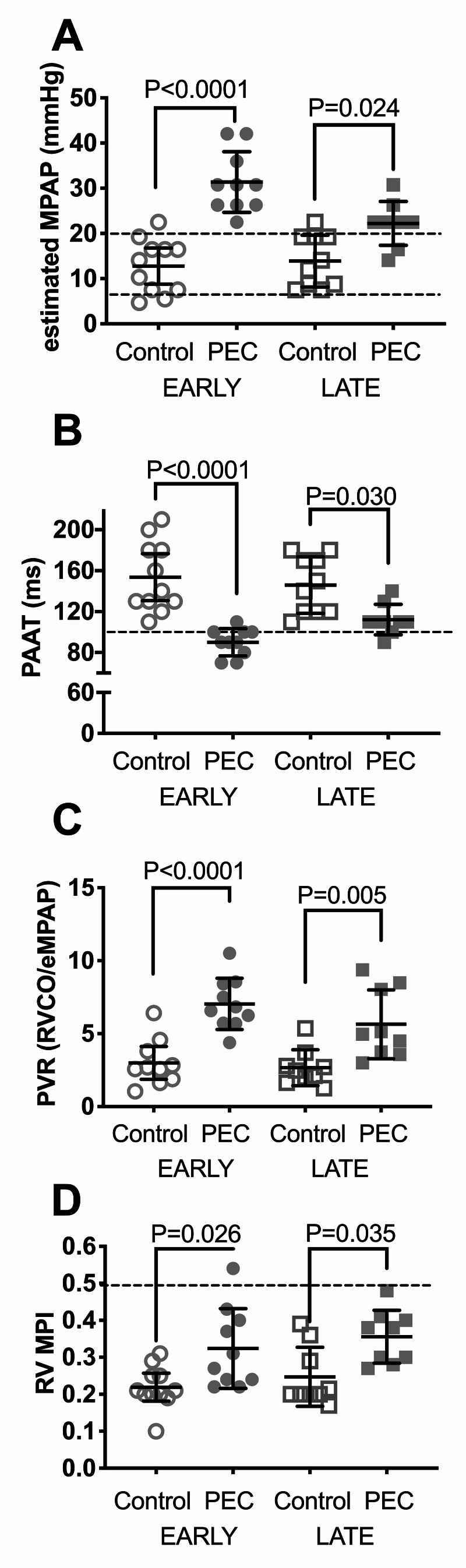
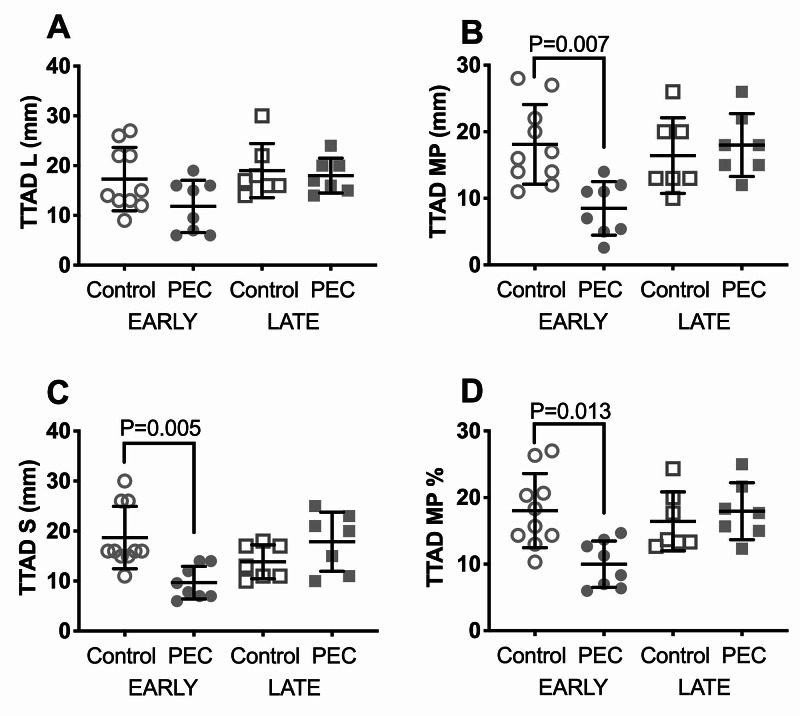
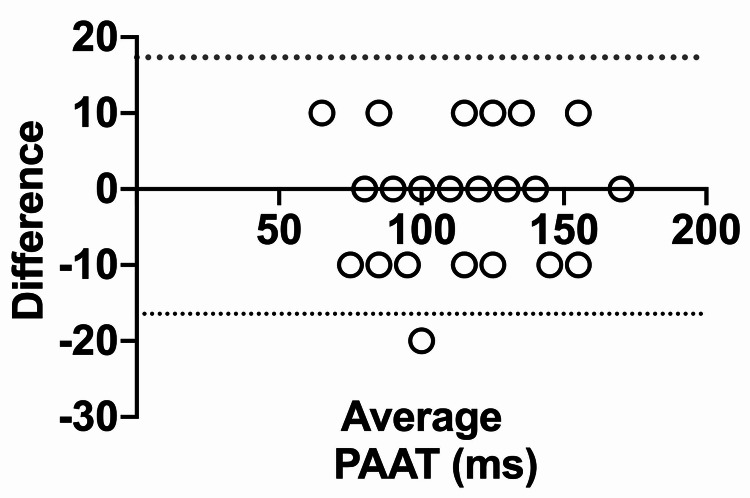
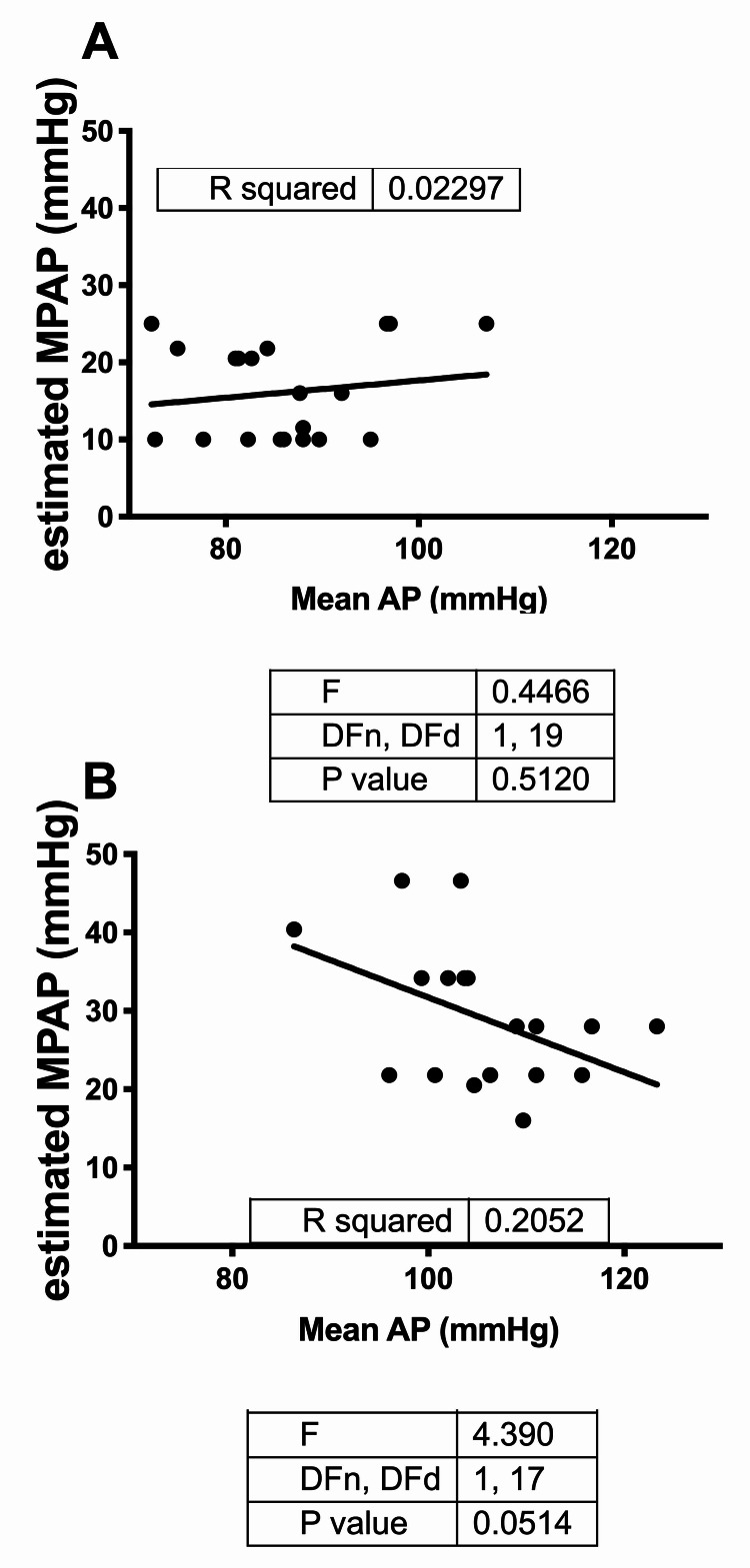
Background and objective Pre-eclampsia (PEC) is associated with the release of anti-angiogenic factors that are incriminated in raising systemic and pulmonary vascular resistance (PVR). Compared to the left heart and systemic circulation, much less attention has been paid to the right heart and pulmonary circulation in patients with PEC. We used transthoracic echocardiography (TTE) to estimate pulmonary artery (PA) pressure and right ventricular (RV) function in women with PEC. Materials and methods We conducted a case-control study at a tertiary care academic center. Ten early PEC (<34-week gestation) and nine late PEC (≥34-week gestation) patients with 11 early and 10 late gestational age-matched controls were enrolled. Two-dimensional TTE was performed on all patients. The estimated mean PA pressure (eMPAP) was calculated based on PA acceleration time (PAAT). PVR was estimated from eMPAP and RV cardiac output (RV CO). RV myocardial performance index (RV MPI), tricuspid annular plane systolic excursion (TAPSE), tissue tricuspid annular displacement (TTAD), and lateral tricuspid annular tissue peak systolic velocity (S') were measured. Results Compared to early controls, in early PEC, the eMPAP and estimated PVR (ePVR) were elevated, PAAT was reduced, RV MPI was increased, TTAD was reduced, and TAPSE and TV S' were unchanged. Compared to late controls, in late PEC, the eMPAP and ePVR were elevated, PAAT was reduced, and RV MPI was increased, while TAPSE, TTAD, and TV S' were unchanged. Conclusions In a sample of women with PEC, early PEC was found to be associated with increased eMPAP and ePVR and subclinical decrement of RV function as assessed by TTE. TTE may be a useful noninvasive screening tool for early detection of pulmonary hypertension and RV dysfunction in PEC. An adequately powered longitudinal study is needed to determine the implications of these findings on long-term outcomes.
Keywords: echo cardiogram; multifactorial pulmonary hypertension; pre-eclampsia.
Copyright © 2021, F. Zaky et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Right ventricular outflow tract Doppler flow analysis and pulmonary arterial coupling by transthoracic echocardiography in sepsis: a retrospective exploratory study.Crit Care. 2022 Oct 3;26(1):303. doi: 10.1186/s13054-022-04160-4. Crit Care. 2022. PMID: 36192793 Free PMC article.
-
High-Resolution Transthoracic Echocardiography Accurately Detects Pulmonary Arterial Pressure and Decreased Right Ventricular Contractility in a Mouse Model of Pulmonary Fibrosis and Secondary Pulmonary Hypertension.J Am Heart Assoc. 2022 Dec 6;11(23):e018353. doi: 10.1161/JAHA.120.018353. Epub 2022 Nov 16. J Am Heart Assoc. 2022. PMID: 36382959 Free PMC article.
-
Echocardiographic assessment of right ventricular function in inferior wall myocardial infarction and angiographic correlation to proximal right coronary artery stenosis.Indian Heart J. 2013 Sep-Oct;65(5):522-8. doi: 10.1016/j.ihj.2013.08.021. Epub 2013 Sep 14. Indian Heart J. 2013. PMID: 24206875 Free PMC article.
-
[Association between echocardiography derived right ventricular function parameters with cardiac magnetic resonance derived right ventricular ejection fraction and 6-minute walk distance in pulmonary hypertension patients].Zhonghua Xin Xue Guan Bing Za Zhi. 2014 Sep;42(9):748-52. Zhonghua Xin Xue Guan Bing Za Zhi. 2014. PMID: 25511095 Chinese.
-
Transthoracic echocardiography in the evaluation of pediatric pulmonary hypertension and ventricular dysfunction.Pulm Circ. 2016 Mar;6(1):15-29. doi: 10.1086/685051. Pulm Circ. 2016. PMID: 27162612 Free PMC article. Review.
Cited by
-
Abnormal Venous Flow in Pregnant Women with Mild Right Ventricular Dysfunction in Repaired Tetralogy of Fallot: A Clinical Model for Organ Dysfunction in Preeclampsia.J Clin Med. 2024 Dec 30;14(1):142. doi: 10.3390/jcm14010142. J Clin Med. 2024. PMID: 39797225 Free PMC article.
References
-
- Pregnancy-related mortality in the United States, 2006-2010. Creanga AA, Berg CJ, Syverson C, Seed K, Bruce FC, Callaghan WM. Obstet Gynecol. 2015;125:5–12. - PubMed
-
- Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. No authors listed. Obstet Gynecol. 2013;122:1122–1131. - PubMed
-
- The rising burden of preeclampsia in the United States impacts both maternal and child health. Shih T, Peneva D, Xu X, et al. Am J Perinatol. 2016;33:329–338. - PubMed
-
- Secular trends in the rates of preeclampsia, eclampsia, and gestational hypertension, United States, 1987-2004. Wallis AB, Saftlas AF, Hsia J, Atrash HK. Am J Hypertens. 2008;21:521–526. - PubMed
-
- The opposing roles of anti-angiogenic factors in cancer and preeclampsia. Gilbert JS, Bauer AJ, Gilbert SA, Banek CT. Front Biosci (Elite Ed) 2012;4:2652–2669. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials