

Do Probiotics During In-Hospital Antibiotic Treatment Prevent Colonization of Gut Microbiota With Multi-Drug-Resistant Bacteria? A Randomized Placebo-Controlled Trial Comparing Saccharomyces to a Mixture of Lactobacillus, Bifidobacterium, and Saccharomyces
- PMID: 33763399
- PMCID: PMC7982943
- DOI: 10.3389/fpubh.2020.578089
Do Probiotics During In-Hospital Antibiotic Treatment Prevent Colonization of Gut Microbiota With Multi-Drug-Resistant Bacteria? A Randomized Placebo-Controlled Trial Comparing Saccharomyces to a Mixture of Lactobacillus, Bifidobacterium, and Saccharomyces
Abstract
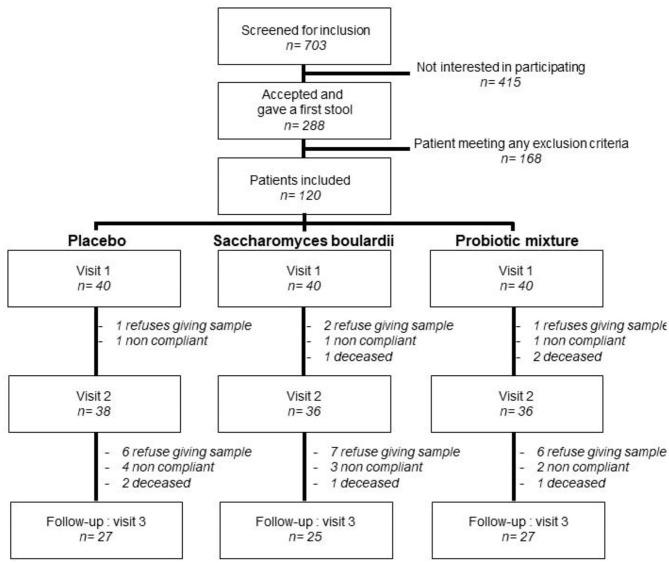
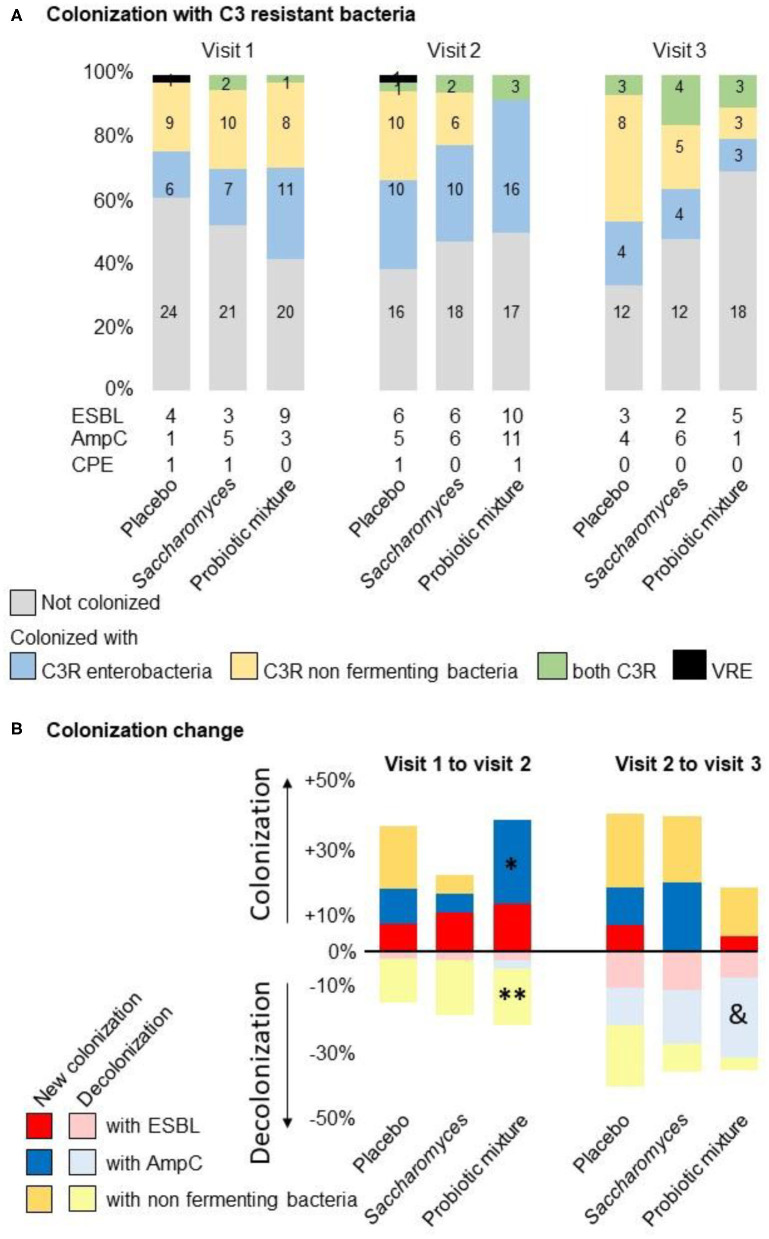
Objective: Most infections with Enterobacteriaceae producing AmpC β-lactamase (AmpC)-, extended-spectrum β-lactamase (ESBL)-, and carbapenemase-producing bacteria, vancomycin-resistant Enterococcus as well as naturally resistant non-fermenting bacteria such as Pseudomonas aeruginosa, are related to a prior colonization of the gut microbiota. The objective of this study was to determine whether treatment with probiotics during an antibiotic treatment could prevent the colonization of the gut microbiota with multi-drug resistant bacteria. Method: In total, 120 patients treated for 10 days with amoxicillin-clavulanate antibiotics were included in a randomized, placebo-controlled, double-blinded trial, comparing the effects of a 30 days treatment with placebo Saccharomyces boulardii CNCM I-745® and a probiotic mixture containing Saccharomyces boulardii, Lactobacillus acidophilus NCFM, Lactobacillus paracasei Lpc-37, Bifidobacterium lactis Bl-04, and Bifidobacterium lactis Bi-07 (Bactiol duo®). Study treatment was initiated within 48 h of the antibiotic being initiated. Most of the patients included were elderly with a mean age of 78 years old with multiple comorbidities. Stools were collected at the time of inclusion in the trial, at the end of the antibiotic treatment, and the end of the study treatment. These were cultured on selective antibiotic media. Results: Treatment with the probiotic mixture led to a significant decline in colonization with Pseudomonas after antibiotic treatment from 25 to 8.3% (p = 0.041). Colonization with AmpC-producing enterobacteria was transiently increased after the antibiotic treatment (p = 0.027) and declined after the probiotic intervention (p= 0.041). No significant changes were observed in the placebo and Saccharomyces groups. Up to 2 years after the trial, no infection with ESBL-producing bacteria was observed in the probiotic mixture group. Conclusion: The association of Saccharomyces boulardii with specific strains of Lactobacillus and Bifidobacterium influences antibiotic treatment by counteracting the colonization of the colon microbiota with antibiotic-resistant pathogens.
Keywords: AmpC & [beta]-lactamase; antibiotic resistance; clinics and hospitals; extended-spectrum beta-lactamase; microbiota; prevention; probiotics; pseudomonas.
Copyright © 2021 Wieërs, Verbelen, Van Den Driessche, Melnik, Vanheule, Marot and Cani.
Conflict of interest statement
GW reports grants from Metagenics, during the conduct of the study. MV and GV reports non-financial support from Metagenics Europe, during the conduct of the study and an employee of Metagenics Europe, distributor of Bactiol duo used in this trial. PC is inventor on patent applications dealing with the use of A.muciniphila and its components in the treatment of obesity and related disorders and co-founder of A-Mansia biotech SA. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Thaden JT, Park LP, Maskarinec SA, Ruffin F, Fowler VG, Jr, van Duin D. Results from a 13-year prospective cohort study show increased mortality associated with bloodstream infections caused by Pseudomonas aeruginosa compared to other bacteria. Antimicrob Agents Chemother. (2017) 61:e02671–16. 10.1128/AAC.02671-16 - DOI - PMC - PubMed
-
- Kang CI, Chung DR, Ko KS, Peck KR, Song JH, Korean Network for Study of Infectious D . Risk factors for infection and treatment outcome of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae bacteremia in patients with hematologic malignancy. Ann Hematol. (2012) 91:115–21. 10.1007/s00277-011-1247-7 - DOI - PubMed
-
- Shamsrizi P, Gladstone BP, Carrara E, Luise D, Cona A, Bovo C, et al. Variation of effect estimates in the analysis of mortality and length of hospital stay in patients with infections caused by bacteria-producing extended-spectrum beta-lactamases: a systematic review and meta-analysis. BMJ Open. (2020) 10:e030266. 10.1136/bmjopen-2019-030266 - DOI - PMC - PubMed
-
- Golzarri MF, Silva-Sanchez J, Cornejo-Juarez P, Barrios-Camacho H, Chora-Hernández LD, Velázquez-Acosta C, et al. Colonization by fecal extended-spectrum beta-lactamase-producing Enterobacteriaceae and surgical site infections in patients with cancer undergoing gastrointestinal and gynecologic surgery. Am J Infect Control. (2019) 47:916–21. 10.1016/j.ajic.2019.01.020 - DOI - PubMed
-
- Ruppe E, Lixandru B, Cojocaru R, Büke C, Paramythiotou E, Angebault C, et al. Relative fecal abundance of extended-spectrum-beta-lactamase-producing Escherichia coli strains and their occurrence in urinary tract infections in women. Antimicrob Agents Chemother. (2013) 57:4512–7. 10.1128/AAC.00238-13 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical