

Impact of COVID-19 on exercise pathophysiology: a combined cardiopulmonary and echocardiographic exercise study
- PMID: 33764166
- PMCID: PMC8143785
- DOI: 10.1152/japplphysiol.00710.2020
Impact of COVID-19 on exercise pathophysiology: a combined cardiopulmonary and echocardiographic exercise study
Abstract
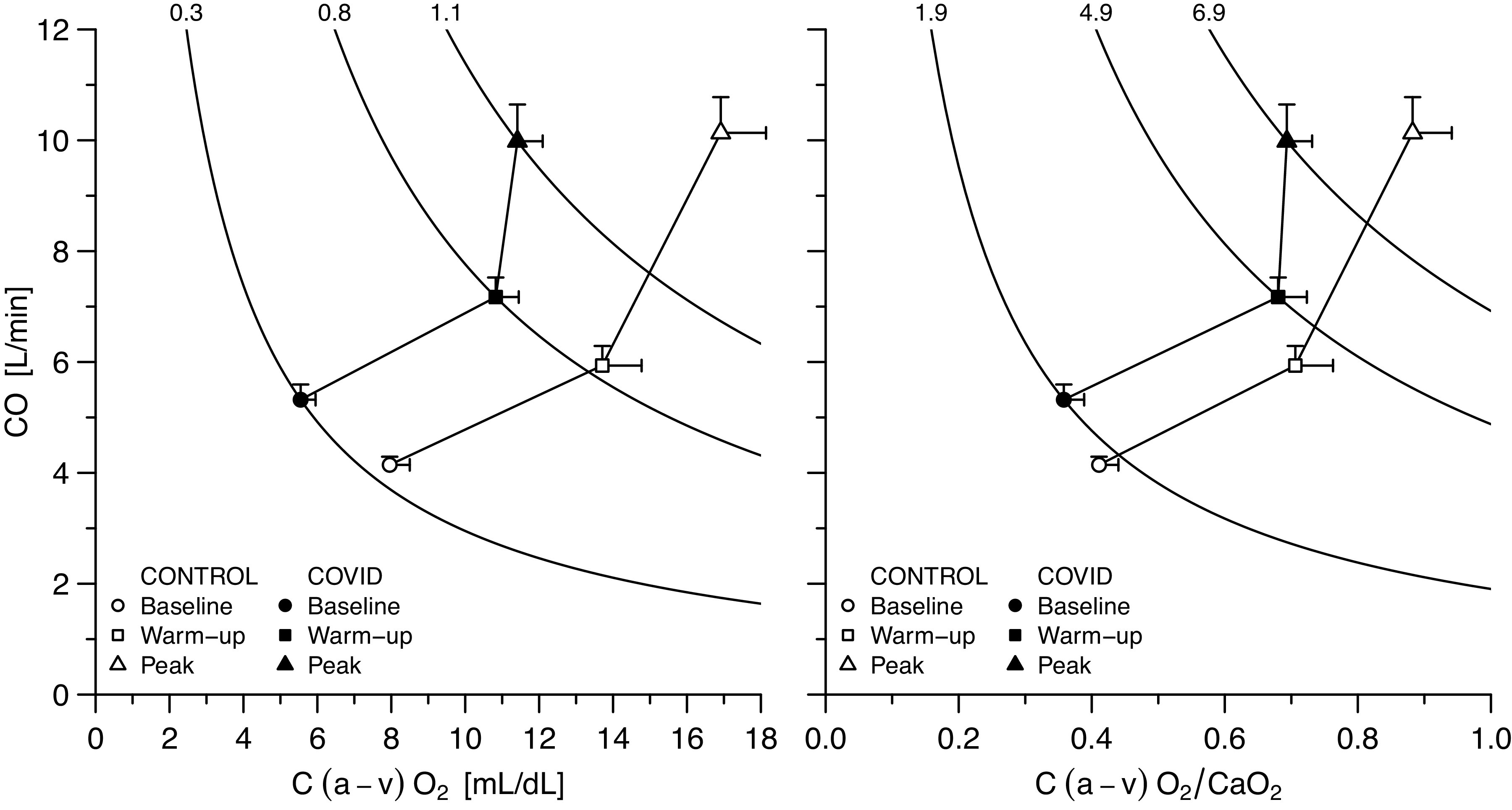
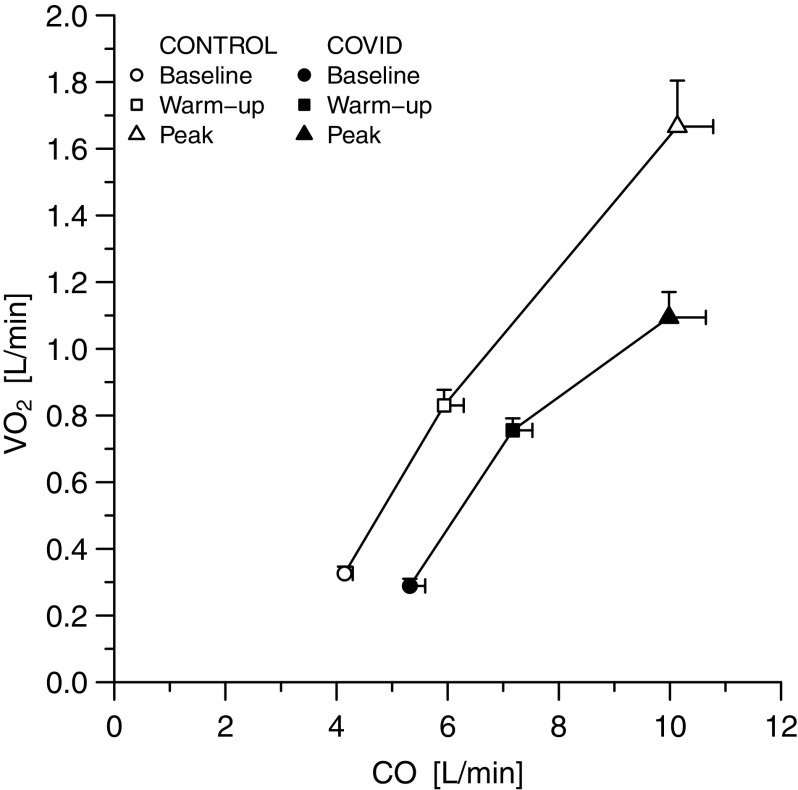
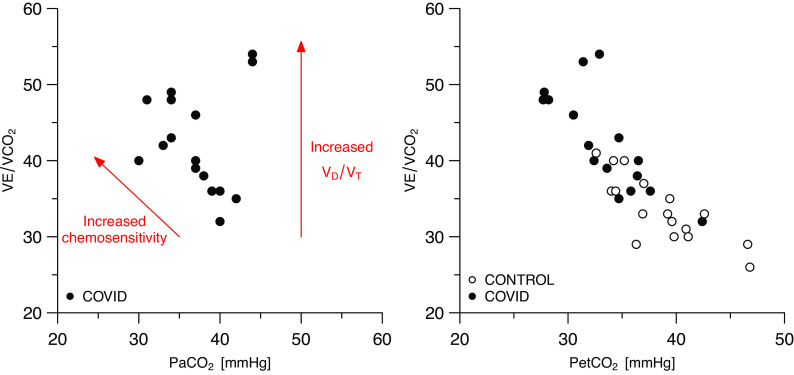
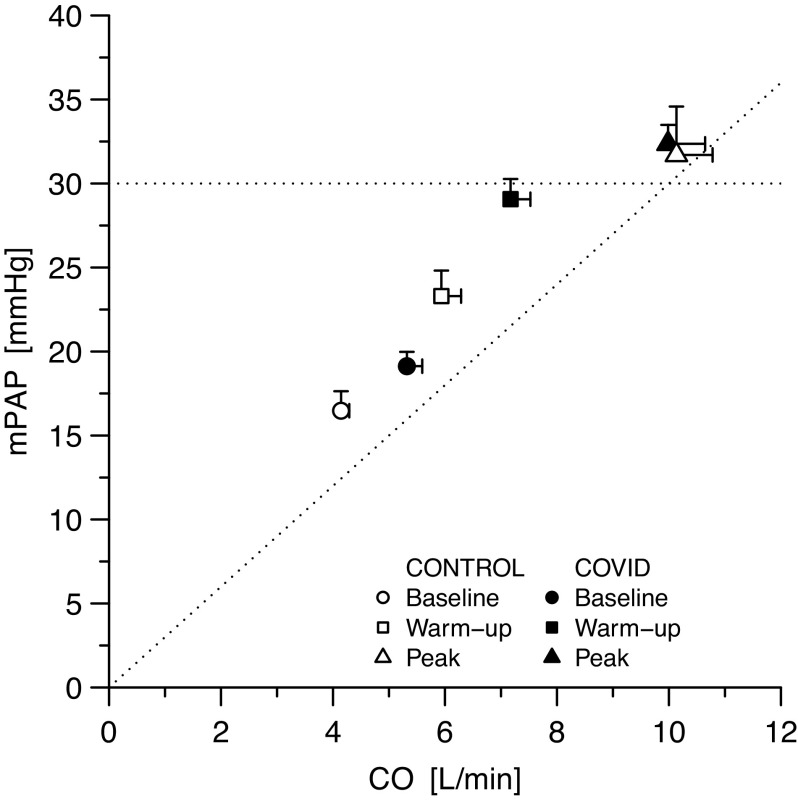
Survivors from COVID-19 pneumonia can present with persisting multisystem involvement (lung, pulmonary vessels, heart, muscle, red blood cells) that may negatively affect exercise capacity. We sought to determine the extent and the determinants of exercise limitation in patients with COVID-19 at the time of hospital discharge. Eighteen consecutive patients with COVID-19 and 1:1 age-, sex-, and body mass index-matched controls underwent: spirometry, echocardiography, cardiopulmonary exercise test and exercise echocardiography for the study of pulmonary circulation. Arterial blood was sampled at rest and during exercise in patients with COVID-19. Patients with COVID-19 lie roughly on the same oxygen consumption isophlets than controls both at rest and during submaximal exercise, thanks to supernormal cardiac output (P < 0.05). Oxygen consumption at peak exercise was reduced by 30% in COVID-19 (P < 0.001), due to a peripheral extraction limit. In addition, within COVID-19 patients, hemoglobin content was associated with peak oxygen consumption (R2 = 0.46, P = 0.002). Respiratory reserve was not exhausted (median [IRQ], 0.59 [0.15]) in spite of moderate reduction of forced vital capacity (79 ± 40%). Pulmonary artery pressure increase during exercise was not different between patients and controls. Ventilatory equivalents for carbon dioxide were higher in patients with COVID-19 than in controls (39.5 [8.5] vs. 29.5 [8.8], P < 0.001), and such an increase was mainly explained by increased chemosensitivity. When recovering from COVID-19, patients present with reduced exercise capacity and augmented exercise hyperventilation. Peripheral factors, including anemia and reduced oxygen extraction by peripheral muscles were the major determinants of deranged exercise physiology. Pulmonary vascular function seemed unaffected, despite restrictive lung changes.NEW & NOTEWORTHY At the time of hospital discharge, patients with COVID-19 present with reduced functional capacity and exercise hyperventilation. Peripheral factors, namely reduced oxygen extraction (myopathy) and anemia, which are not fully compensated by a supernormal cardiac output response, account for exercise limitation before exhaustion of the respiratory reserve. Enhanced chemoreflex sensitivity, rather increased dead space, mainly accounts for exercise hyperventilation. The pulmonary vascular response to exercise circulation of survived patients with COVID-19 does not present major pathological changes.
Keywords: COVID-19; cardiopulmonary exercise test; echocardiography; hemodynamics.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- World Health Organization. Coronavirus disease (COVID-19) pandemic (Online). https://www.who.int/emergencies/diseases/novel-coronavirus-2019. [20 February 2021].
-
- van Dam LF, Kroft LJM, van der Wal LI, Cannegieter SC, Eikenboom J, de Jonge E, Huisman MV, Klok FA. Clinical and computed tomography characteristics of COVID-19 associated acute pulmonary embolism: a different phenotype of thrombotic disease? Thromb Res 193: 86–89, 2020. doi: 10.1016/j.thromres.2020.06.010. - DOI - PMC - PubMed
-
- Ackermann M, Verleden SE, Kuehnel M, Haverich A, Welte T, Laenger F, Vanstapel A, Werlein C, Stark H, Tzankov A, Li WW, Li VW, Mentzer SJ, Jonigk D. Pulmonary vascular endothelialitis, thrombosis, and angiogenesis in Covid-19. N Engl J Med 383: 120–128, 2020. doi: 10.1056/NEJMoa2015432. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical