

Assessment of a Risk-Based Approach for Triaging Mammography Examinations During Periods of Reduced Capacity
- PMID: 33764423
- PMCID: PMC7994953
- DOI: 10.1001/jamanetworkopen.2021.1974
Assessment of a Risk-Based Approach for Triaging Mammography Examinations During Periods of Reduced Capacity
Abstract
Importance: Breast cancer screening, surveillance, and diagnostic imaging services were profoundly limited during the initial phase of the coronavirus disease 2019 (COVID-19) pandemic.
Objective: To develop a risk-based strategy for triaging mammograms during periods of decreased capacity.
Design, setting, and participants: This population-based cohort study used data collected prospectively from mammography examinations performed in 2014 to 2019 at 92 radiology facilities in the Breast Cancer Surveillance Consortium. Participants included individuals undergoing mammography. Data were analyzed from August 10 to November 3, 2020.
Exposures: Clinical indication for screening, breast symptoms, personal history of breast cancer, age, time since last mammogram/screening interval, family history of breast cancer, breast density, and history of high-risk breast lesion.
Main outcomes and measures: Combinations of clinical indication, clinical history, and breast cancer risk factors that subdivided mammograms into risk groups according to their cancer detection rate were identified using classification and regression trees.
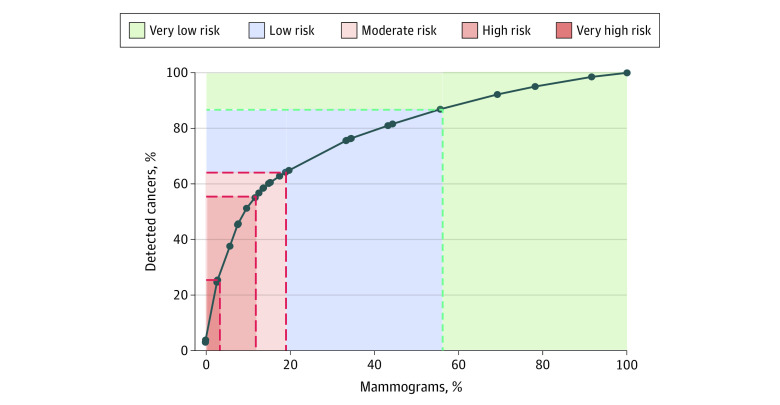
Results: The cohort included 898 415 individuals contributing 1 878 924 mammograms (mean [SD] age at mammogram, 58.6 [11.2] years) interpreted by 448 radiologists, with 1 722 820 mammograms in individuals without a personal history of breast cancer and 156 104 mammograms in individuals with a history of breast cancer. Most individuals were aged 50 to 69 years at imaging (1 113 174 mammograms [59.2%]), and 204 305 (11.2%) were Black, 206 087 (11.3%) were Asian or Pacific Islander, 126 677 (7.0%) were Hispanic or Latina, and 40 021 (2.2%) were another race/ethnicity or mixed race/ethnicity. Cancer detection rates varied widely based on clinical indication, breast symptoms, personal history of breast cancer, and age. The 12% of mammograms with very high (89.6 [95% CI, 82.3-97.5] to 122.3 [95% CI, 108.1-138.0] cancers detected per 1000 mammograms) or high (36.1 [95% CI, 33.1-39.3] to 47.5 [95% CI, 42.4-53.3] cancers detected per 1000 mammograms) cancer detection rates accounted for 55% of all detected cancers and included mammograms to evaluate an abnormal mammogram or breast lump in individuals of all ages regardless of breast cancer history, to evaluate breast symptoms other than lump in individuals with a breast cancer history or without a history but aged 60 years or older, and for short-interval follow-up in individuals aged 60 years or older without a breast cancer history. The 44.2% of mammograms with very low cancer detection rates accounted for 13.1% of detected cancers and included annual screening mammograms in individuals aged 50 to 69 years (3.8 [95% CI, 3.5-4.1] cancers detected per 1000 mammograms) and all screening mammograms in individuals younger than 50 years regardless of screening interval (2.8 [95% CI, 2.6-3.1] cancers detected per 1000 mammograms).
Conclusions and relevance: In this population-based cohort study, clinical indication and individual risk factors were associated with cancer detection and may be useful for prioritizing mammography in times and settings of decreased capacity.
Conflict of interest statement
Figures
Comment in
-
Selecting Patients for Mammographic Evaluation Based on Breast Cancer Risk During the COVID-19 Pandemic.JAMA Netw Open. 2021 Mar 1;4(3):e212546. doi: 10.1001/jamanetworkopen.2021.2546. JAMA Netw Open. 2021. PMID: 33764418 No abstract available.
References
-
- Epic Health Research Network . Delayed cancer screenings. Accessed February 15, 2021. https://ehrn.org/articles/delays-in-preventive-cancer-screenings-during-...
-
- Martin K, Kurowski D, Given P, Kennedy K, Clayton E. The impact of COVID-19 on the use of preventive health care. Health Care Cost Institute. December 18, 2020. Accessed February 10, 2021. https://healthcostinstitute.org/hcci-research/the-impact-of-covid-19-on-...
-
- DePolo J. COVID-19 pandemic delayed breast cancer screening in many parts of the United States. BreastCancer.org. July 30, 2020. Accessed February 10, 2021. https://www.breastcancer.org/research-news/covid-19-delayed-screening-in-us
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
