

Liver stiffness by magnetic resonance elastography is associated with increased risk of cardiovascular disease in patients with non-alcoholic fatty liver disease
- PMID: 33764550
- PMCID: PMC8514119
- DOI: 10.1111/apt.16324
Liver stiffness by magnetic resonance elastography is associated with increased risk of cardiovascular disease in patients with non-alcoholic fatty liver disease
Abstract
Background: Magnetic resonance elastography (MRE) is a reliable non-invasive alternative to liver biopsy for assessing liver fibrosis. There are limited data regarding an association between liver fibrosis by MRE and risk of cardiovascular disease (CVD).
Aim: To investigate the association of high-risk CVD phenotype determined by coronary artery calcification (CAC) with liver fibrosis by MRE in patients with non-alcoholic fatty liver disease (NAFLD).
Method: This was a cross-sectional analysis of well-characterised, prospective cohorts including 105 patients with NAFLD (MR imaging-derived proton density fat fraction ≥ 5%) with contemporaneous cardiac computed tomography (CT) and MRE. Patients were assessed using MRE for liver stiffness, and cardiac CT for the presence of CAC (defined as coronary artery calcium score > 0). Odds of presence of CAC were analysed using logistic regression analysis.
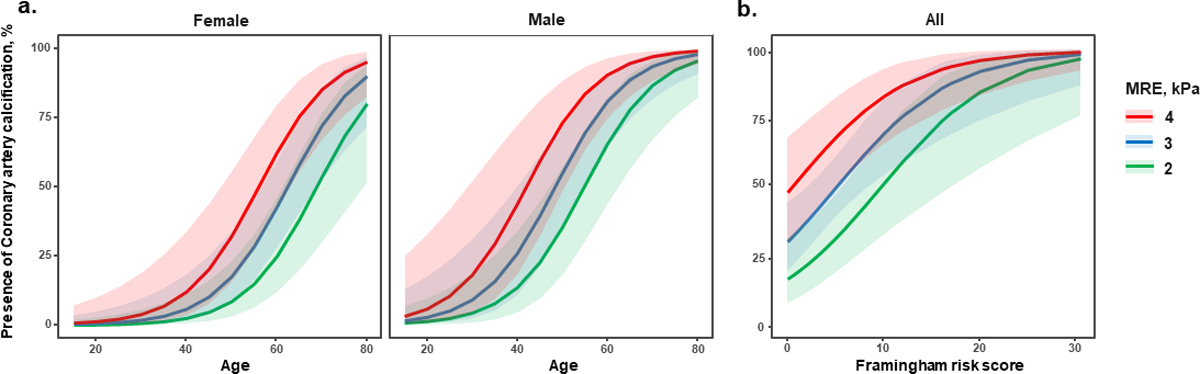
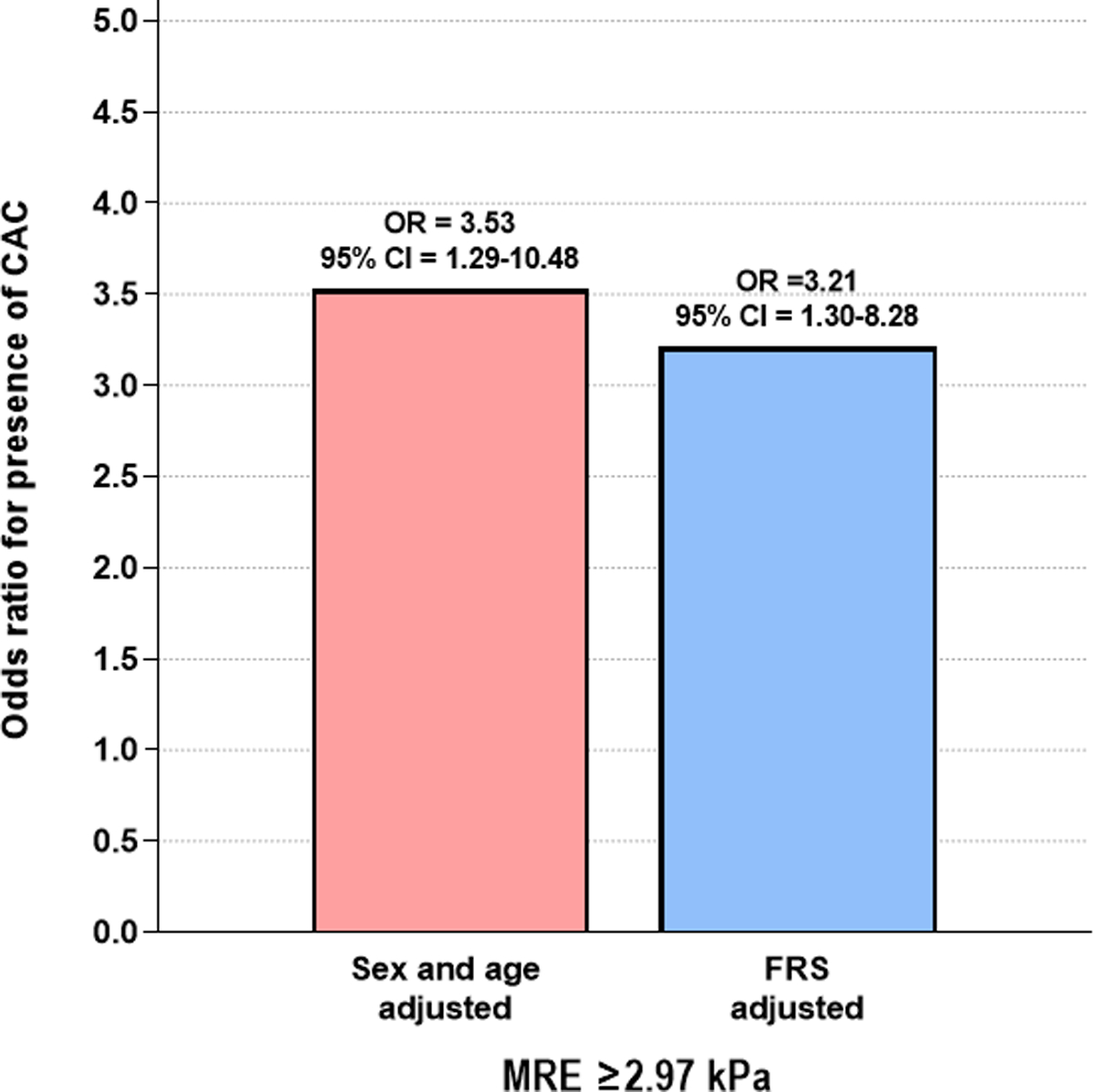
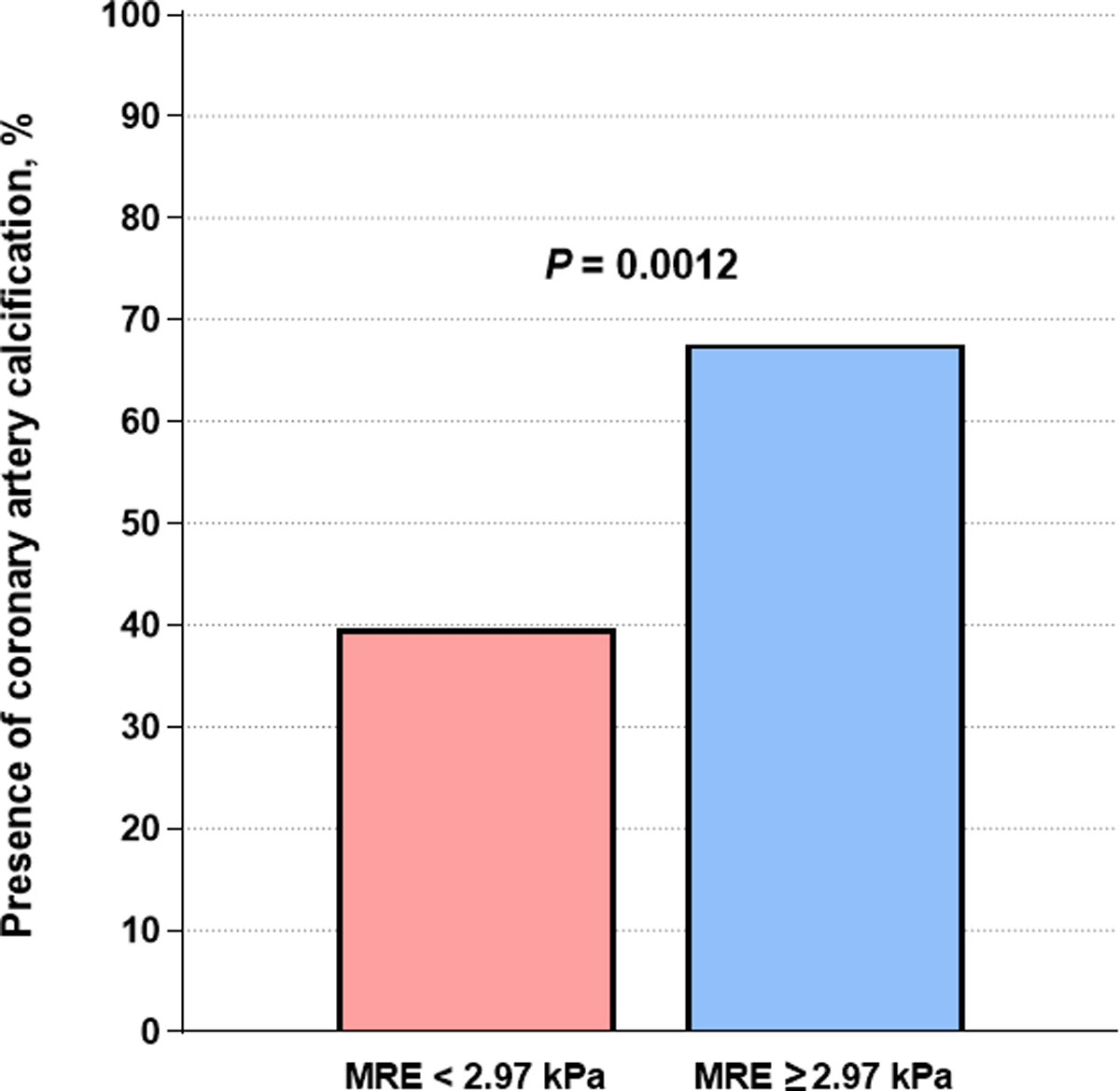
Results: The average age and body mass index were 54.9 years and 32.9 kg/m2 respectively. In this cohort, 49.5% of patients had CAC and 35.2% had significant liver fibrosis (defined as MRE ≥2.97 kPa). Compared to patients without CAC, those with CAC were older (50.0 [39.0-59.0] vs 63.0 [55.5-67.5], P < 0.001) and had higher Framingham risk score (FRS, 1.0 [0.5-3.5] vs 6.0 [2.0-12.0], P < 0.001). In multivariable-adjusted analysis, liver stiffness as a continuous trait on MRE was independently associated with the presence of CAC in a sex and age-adjusted model (adjusted odd ratios [aOR] = 2.23, 95% confidence interval [CI] = 1.31-4.34, P = 0.007) as well as in a FRS-adjusted model (aOR = 2.16, 95% CI = 1.29-4.09, P = 0.008). When analysed as a dichotomous trait, significant fibrosis (MRE-stiffness ≥2.97 kPa) remained independently associated with the presence of CAC in both FRS-adjusted model and sex and age-adjusted model (aOR = 3.21-3.53, P = 0.013-0.017). In addition, CAC was more prevalent in patients with significant fibrosis than those without as determined by MRE (67.6% vs 39.7%, P = 0.012).
Conclusion: Liver stiffness determined by MRE is an independent predictor for the presence of CAC in patients with NAFLD. Patients with NAFLD and significant fibrosis by MRE should be considered for further cardiovascular risk assessment, regardless of their FRS.
© 2021 John Wiley & Sons Ltd.
Figures
Comment in
-
Editorial: liver stiffness by magnetic resonance elastography and cardiovascular risk in non-alcoholic fatty liver disease-simply associated or more complicated? Authors' reply.Aliment Pharmacol Ther. 2021 Jun;53(11):1230-1231. doi: 10.1111/apt.16364. Aliment Pharmacol Ther. 2021. PMID: 33961702 No abstract available.
-
Editorial: liver stiffness by magnetic resonance elastography and cardiovascular risk in non-alcoholic fatty liver disease-simply associated or more complicated?Aliment Pharmacol Ther. 2021 Jun;53(11):1228-1229. doi: 10.1111/apt.16350. Aliment Pharmacol Ther. 2021. PMID: 33961704 No abstract available.
-
Letter: coronary atherosclerosis in patients with significant hepatic fibrosis in non-alcoholic fatty liver disease-the role for non-invasive testing.Aliment Pharmacol Ther. 2021 Jul;54(2):214-215. doi: 10.1111/apt.16435. Aliment Pharmacol Ther. 2021. PMID: 34170537 No abstract available.
-
Letter: coronary atherosclerosis in patients with significant hepatic fibrosis in non-alcoholic fatty liver disease-a realm for non-invasive testing. Authors' reply.Aliment Pharmacol Ther. 2021 Jul;54(2):216. doi: 10.1111/apt.16462. Aliment Pharmacol Ther. 2021. PMID: 34170539 No abstract available.
References
-
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol 2013;10(11):686–690. - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67(1):328–357. - PubMed
-
- Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017;66(6):1138–1153. - PubMed
Publication types
MeSH terms
Grants and funding
- U01DK061734/DK/NIDDK NIH HHS/United States
- 5UL1TR001442/TR/NCATS NIH HHS/United States
- R01DK121378/DK/NIDDK NIH HHS/United States
- P42 ES010337/ES/NIEHS NIH HHS/United States
- R01DK124318/DK/NIDDK NIH HHS/United States
- P30 DK120515/DK/NIDDK NIH HHS/United States
- U01 AA029019/AA/NIAAA NIH HHS/United States
- R01 DK124318/DK/NIDDK NIH HHS/United States
- P30DK120515/DK/NIDDK NIH HHS/United States
- U01 DK061734/DK/NIDDK NIH HHS/United States
- P01 HL147835/HL/NHLBI NIH HHS/United States
- R01 DK121378/DK/NIDDK NIH HHS/United States
- R01 DK106419/DK/NIDDK NIH HHS/United States
- 5P42ES010337/ES/NIEHS NIH HHS/United States
- P01HL147835/HL/NHLBI NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- R01DK106419/DK/NIDDK NIH HHS/United States
- U01AA029019/AA/NIAAA NIH HHS/United States