

Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine - United States, 2003-2018
- PMID: 33764964
- PMCID: PMC7993559
- DOI: 10.15585/mmwr.mm7012a2
Declines in Prevalence of Human Papillomavirus Vaccine-Type Infection Among Females after Introduction of Vaccine - United States, 2003-2018
Erratum in
-
Erratum: Vol. 70, No. 12.MMWR Morb Mortal Wkly Rep. 2021 Apr 2;70(13):502. doi: 10.15585/mmwr.mm7013a6. MMWR Morb Mortal Wkly Rep. 2021. PMID: 33793466 Free PMC article. No abstract available.
Abstract
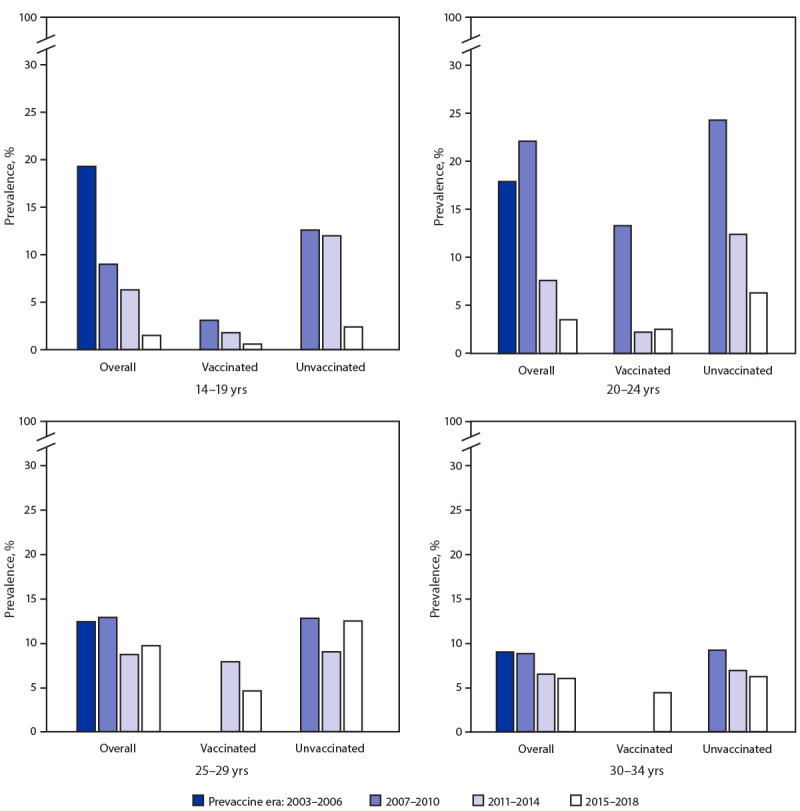
Human papillomavirus (HPV) is the most common sexually transmitted infection in the United States (1). Although most infections resolve without clinical sequalae, persistent HPV infection can cause cervical, other anogenital, and oropharyngeal cancers and anogenital warts. HPV vaccination has been recommended in the United States at age 11-12 years since 2006 for females and since 2011 for males. Catch-up vaccination is recommended through age 26 years.* A quadrivalent vaccine (4vHPV) targeting types 6, 11, 16, and 18 was mainly used until 2015, when a 9-valent vaccine (9vHPV), targeting the same four types as 4vHPV and five additional types (31, 33, 45, 52, and 58), was introduced; 9vHPV has been the only vaccine available in the United States since the end of 2016 (2). HPV vaccination coverage has increased but remains lower than that of other vaccinations recommended for adolescents (3). A decrease in prevalence of 4vHPV types detected in cervicovaginal swabs among young females from the prevaccine era (2003-2006) to 2007-2010 in the National Health and Nutrition Examination Survey (NHANES) was an early indicator of vaccine impact (2) and was also observed in later periods (4,5). NHANES data from 2017-2018 were included in this analysis to update HPV prevalence estimates among females aged 14-34 years. From the prevaccine era to 2015-2018, significant decreases in 4vHPV-type prevalence occurred among females aged 14-19 years (88%) and 20-24 years (81%). In sexually experienced females, 4vHPV-type prevalence decreased in those who reported receiving ≥1 HPV vaccine dose (97% among those aged 14-19 years, 86% among those aged 20-24 years) and in those who reported no vaccination (87% among those aged 14-19 years, 65% among those aged 20-24 years). Significant declines among unvaccinated females suggest herd effects. These data show increasing impact of HPV vaccination in the United States. HPV vaccination is a critical prevention tool against HPV infection, anogenital warts, and HPV-attributable precancers and cancers. HPV vaccination is highly effective and is recommended routinely at age 11-12 years and through 26 years for persons not already vaccinated.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
