

Diagnosis and clinical management of hepatosplenic schistosomiasis: A scoping review of the literature
- PMID: 33764979
- PMCID: PMC7993612
- DOI: 10.1371/journal.pntd.0009191
Diagnosis and clinical management of hepatosplenic schistosomiasis: A scoping review of the literature
Abstract
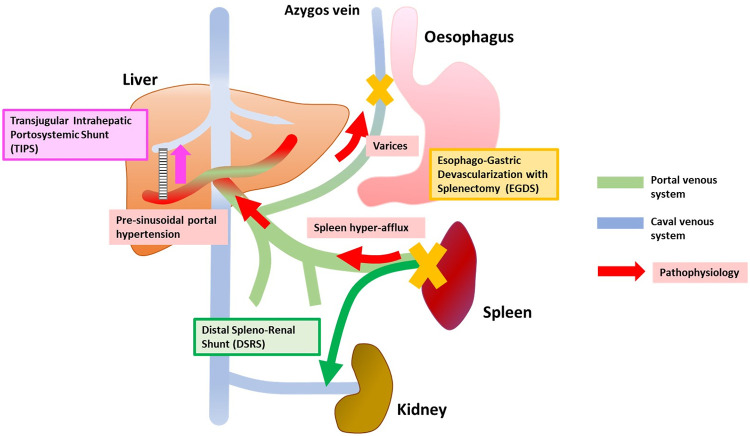
Background: Hepatosplenic schistosomiasis (HSS) is a disease caused by chronic infection with Schistosma spp. parasites residing in the mesenteric plexus; portal hypertension causing gastrointestinal bleeding is the most dangerous complication of this condition. HSS requires complex clinical management, but no specific guidelines exist. We aimed to provide a comprehensive picture of consolidated findings and knowledge gaps on the diagnosis and treatment of HSS.
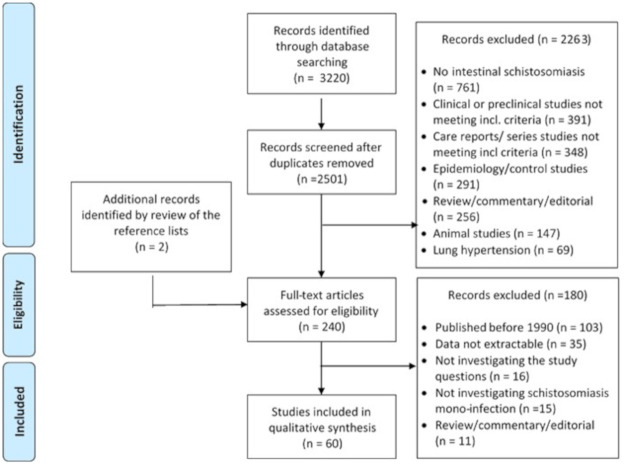
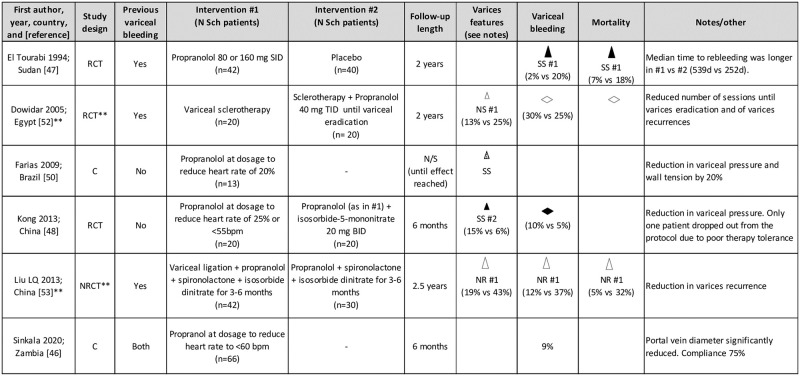
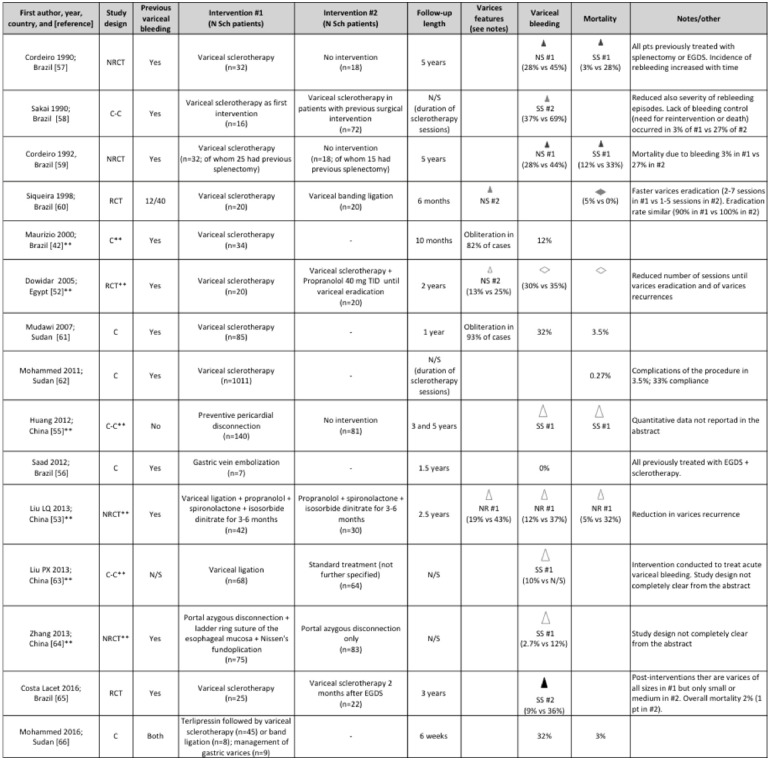
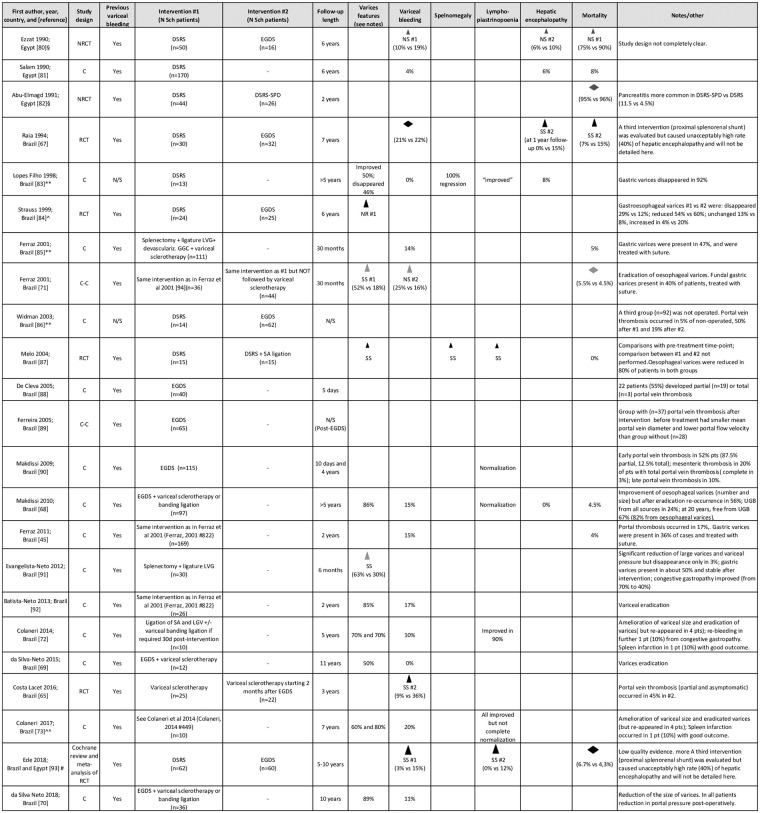
Methodology/principal findings: We reviewed relevant original publications including patients with HSS with no coinfections, published in the past 40 years, identified through MEDLINE and EMBASE databases. Treatment with praziquantel and HSS-associated pulmonary hypertension were not investigated. Of the included 60 publications, 13 focused on diagnostic aspects, 45 on therapeutic aspects, and 2 on both aspects. Results were summarized using effect direction plots. The most common diagnostic approaches to stratify patients based on the risk of variceal bleeding included the use of ultrasonography and platelet counts; on the contrary, evaluation and use of noninvasive tools to guide the choice of therapeutic interventions are lacking. Publications on therapeutic aspects included treatment with beta-blockers, local management of esophageal varices, surgical procedures, and transjugular intrahepatic portosystemic shunt. Overall, treatment approaches and measured outcomes were heterogeneous, and data on interventions for primary prevention of gastrointestinal bleeding and on the long-term follow-up after interventions were lacking.
Conclusions: Most interventions have been developed on the basis of individual groups' experiences and almost never rigorously compared; furthermore, there is a lack of data regarding which parameters can guide the choice of intervention. These results highlight a dramatic need for the implementation of rigorous prospective studies with long-term follow-up in different settings to fill such fundamental gaps, still present for a disease affecting millions of patients worldwide.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Institute of Medicine (US) Forum on Microbial Threats. The Causes and Impacts of Neglected Tropical and Zoonotic Diseases: Opportunities for Integrated Intervention Strategies. Washington (DC): National Academies Press (US); 2011. - PubMed
-
- WHO Expert Committee on the Control of Schistosomiasis (2001): Geneva, Switzerland & World Health Organization. (2002). Prevention and control of schistosomiasis and soil-transmitted helminthiasis: report of a WHO expert committee. World Health Organization. https://apps.who.int/iris/handle/10665/42588. Accessed 15 September 2020. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
