

SARS-COV-2 comorbidity network and outcome in hospitalized patients in Crema, Italy
- PMID: 33765013
- PMCID: PMC7993836
- DOI: 10.1371/journal.pone.0248498
SARS-COV-2 comorbidity network and outcome in hospitalized patients in Crema, Italy
Abstract
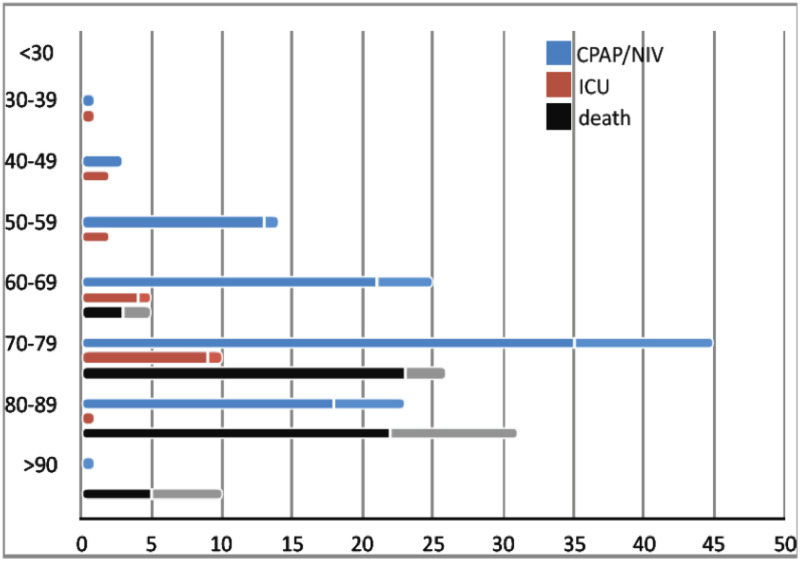
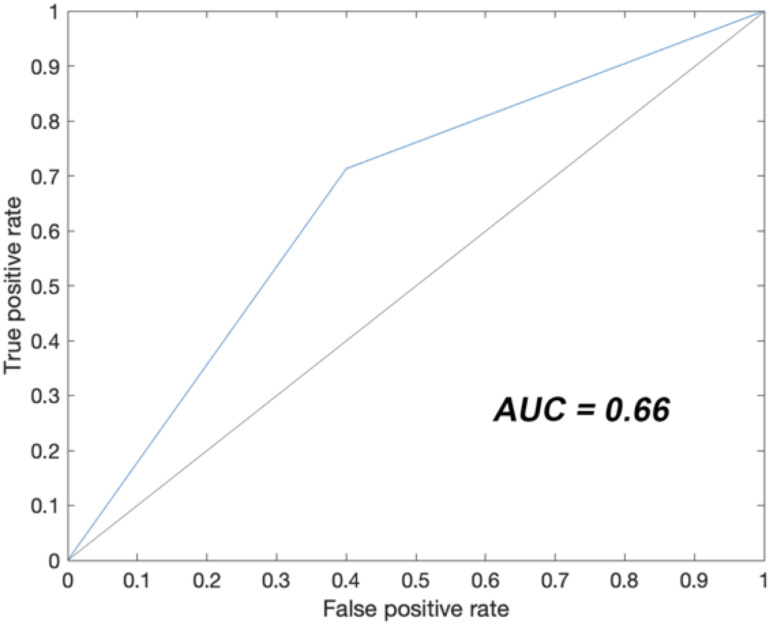
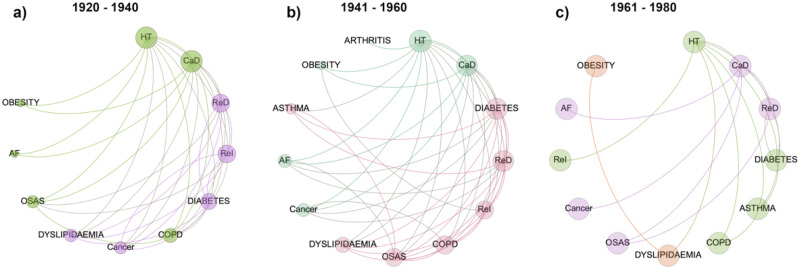
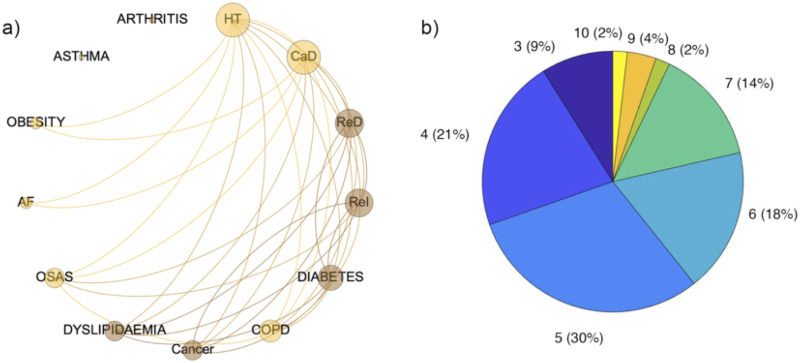
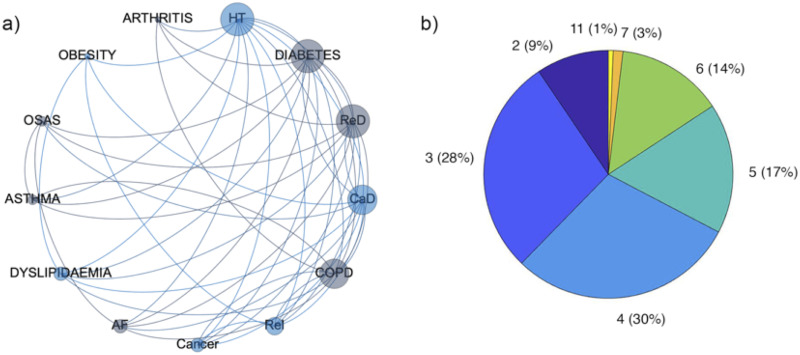
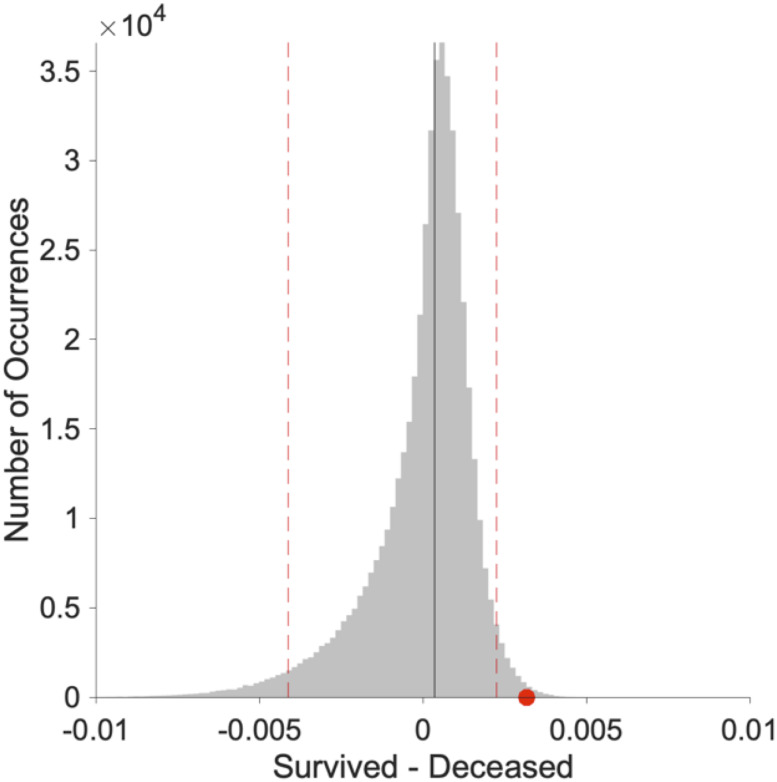
We report onset, course, correlations with comorbidities, and diagnostic accuracy of nasopharyngeal swab in 539 individuals suspected to carry SARS-COV-2 admitted to the hospital of Crema, Italy. All individuals underwent clinical and laboratory exams, SARS-COV-2 reverse transcriptase-polymerase chain reaction on nasopharyngeal swab, and chest X-ray and/or computed tomography (CT). Data on onset, course, comorbidities, number of drugs including angiotensin converting enzyme (ACE) inhibitors and angiotensin-II-receptor antagonists (sartans), follow-up swab, pharmacological treatments, non-invasive respiratory support, ICU admission, and deaths were recorded. Among 411 SARS-COV-2 patients (67.7% males) median age was 70.8 years (range 5-99). Chest CT was performed in 317 (77.2%) and showed interstitial pneumonia in 304 (96%). Fatality rate was 17.5% (74% males), with 6.6% in 60-69 years old, 21.1% in 70-79 years old, 38.8% in 80-89 years old, and 83.3% above 90 years. No death occurred below 60 years. Non-invasive respiratory support rate was 27.2% and ICU admission 6.8%. Charlson comorbidity index and high C-reactive protein at admission were significantly associated with death. Use of ACE inhibitors or sartans was not associated with outcomes. Among 128 swab negative patients at admission (63.3% males) median age was 67.7 years (range 1-98). Chest CT was performed in 87 (68%) and showed interstitial pneumonia in 76 (87.3%). Follow-up swab turned positive in 13 of 32 patients. Using chest CT at admission as gold standard on the entire study population of 539 patients, nasopharyngeal swab had 80% accuracy. Comorbidity network analysis revealed a more homogenous distribution 60-40 aged SARS-COV-2 patients across diseases and a crucial different interplay of diseases in the networks of deceased and survived patients. SARS-CoV-2 caused high mortality among patients older than 60 years and correlated with pre-existing multiorgan impairment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Di Castelnuovo A, COvid-19 RIsk and Treatments (CORIST) Collaboration. Common cardiovascular risk factors and in-hospital mortality in 3,894 patients with COVID-19: survival analysis and machine learning-based findings from the multicentre Italian CORIST Study. Nutr Metab Cardiovasc Dis. 2020;30(11):1899–1913. 10.1016/j.numecd.2020.07.031 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
