

European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care
- PMID: 33765189
- PMCID: PMC7993077
- DOI: 10.1007/s00134-021-06368-4
European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care
Abstract
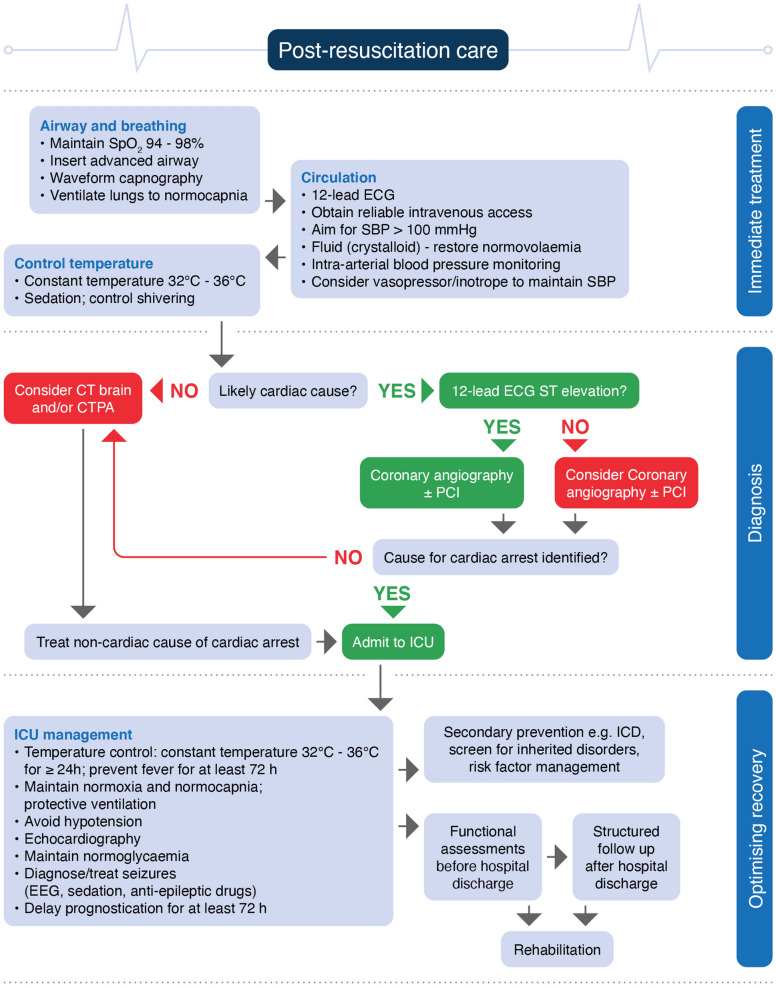
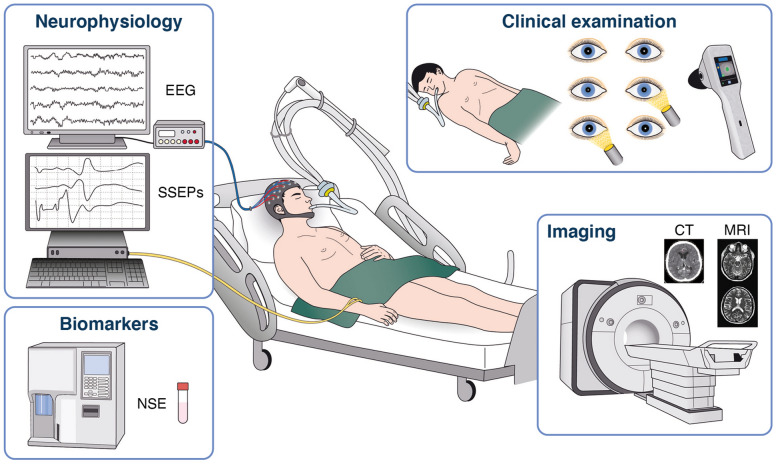
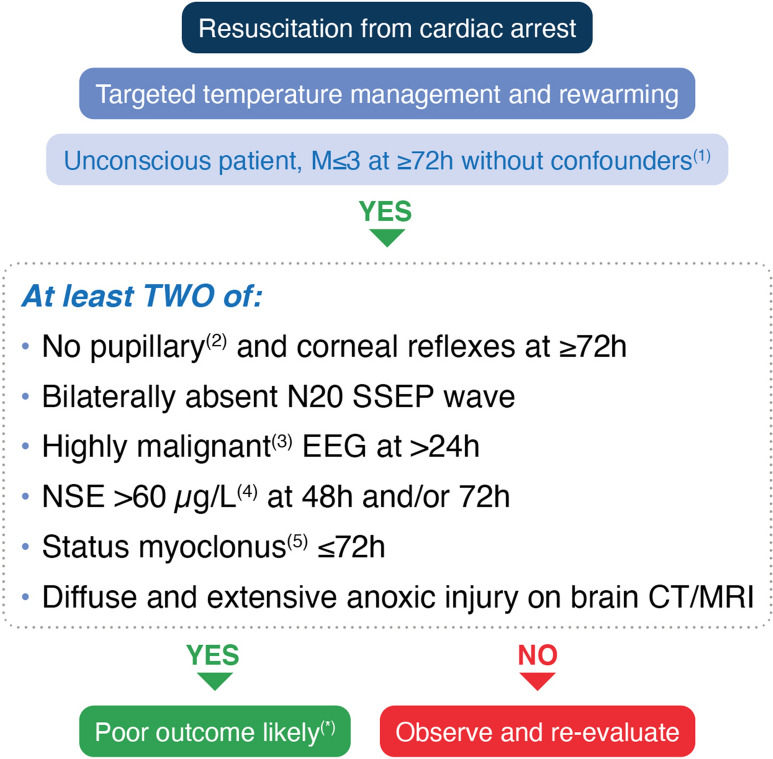
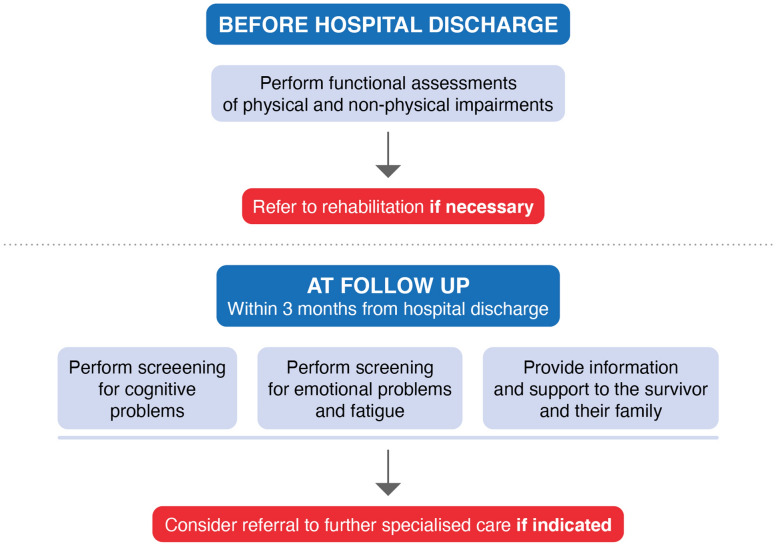
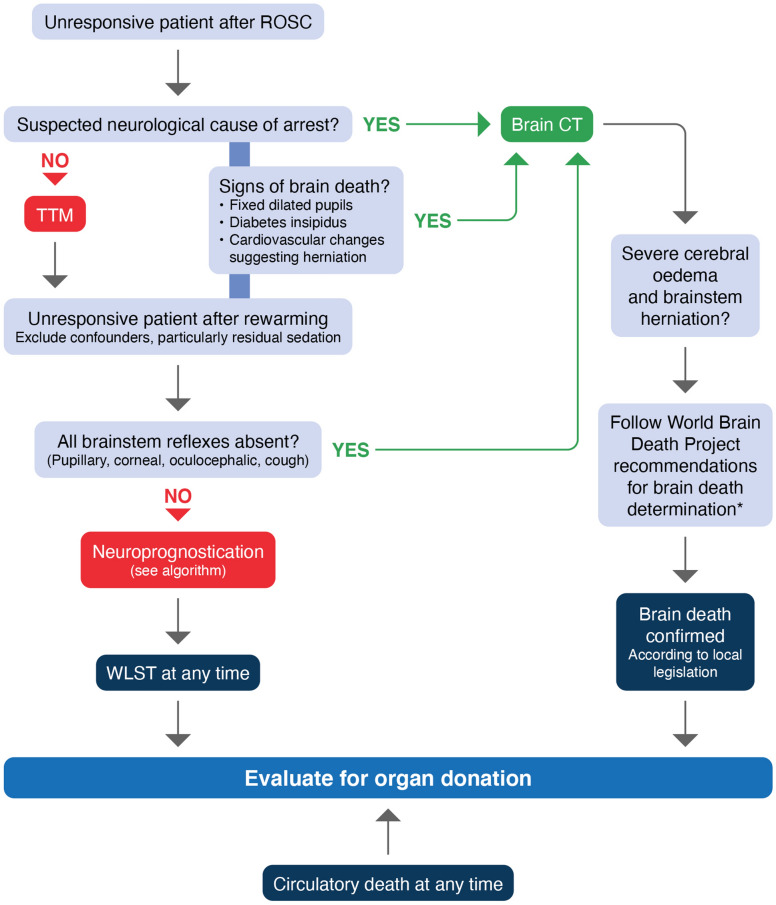
The European Resuscitation Council (ERC) and the European Society of Intensive Care Medicine (ESICM) have collaborated to produce these post-resuscitation care guidelines for adults, which are based on the 2020 International Consensus on Cardiopulmonary Resuscitation Science with Treatment Recommendations. The topics covered include the post-cardiac arrest syndrome, diagnosis of cause of cardiac arrest, control of oxygenation and ventilation, coronary reperfusion, haemodynamic monitoring and management, control of seizures, temperature control, general intensive care management, prognostication, long-term outcome, rehabilitation and organ donation.
Keywords: Cardiac arrest; Guidelines; Post resuscitation care; Prognostication.
Conflict of interest statement
JPN: Editor in Chief Resuscitation. CS: Associate Editor, Intensive Care Medicine. BWB: Treasurer of the European Resuscitation Council (ERC); Chairman of the German Resuscitation Council (GRC); Member of the Advanced Life Support (ALS) Task Force of the International Liaison Committee on Resuscitation (ILCOR); Member of the Executive Committee of the German Interdisciplinary Association for Intensive Care and Emergency Medicine (DIVI), Founder of the Deutsche Stiftung Wiederbelebung; Associate Editor of the European Journal of Anaesthesiology (EJA), Co-Editor of Resuscitation; Editor of Notfall + Rettungsmedizin, Co-Editor of the Brazilian Journal of Anesthesiology. Received fees for lectures from the following companies: Forum für medizinische Fortbildung (FomF), Baxalta Deutschland GmbH, ZOLL Medical Deutschland GmbH, C.R. Bard GmbH, GS Elektromedizinische Geräte G. Stemple GmbH, Novartis Pharma GmbH, Philips GmbH Market DACH, Bioscience Valuation BSV GmbH. AC: Speaker’s Fee from Bard Medical. TC: no conflicts of interest. HF: no conflicts of interest. CG: no conflicts of interest. GL: no conflicts of interest. VRMM: no conflicts of interest. NN: no conflicts of interest. TMO: no conflicts of interest. MBS: Speaker’s Fee from Bard Medical (Ireland). FST: Speaker’s Fees from BD and Zoll. JS: Editor, Resuscitation.
Figures

Comment in
-
"Do no further harm" - Why shall we sedate unresponsive patients?Intensive Care Med. 2021 Jul;47(7):807-808. doi: 10.1007/s00134-021-06422-1. Epub 2021 May 5. Intensive Care Med. 2021. PMID: 33954840 Free PMC article. No abstract available.
-
Why we should sedate unresponsive patients after resuscitation.Intensive Care Med. 2021 Jul;47(7):809-810. doi: 10.1007/s00134-021-06423-0. Epub 2021 May 11. Intensive Care Med. 2021. PMID: 33974108 No abstract available.
References
-
- Nolan JP, Soar J, Cariou A, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines for post-resuscitation Care 2015: section 5 of the European Resuscitation Council Guidelines for Resuscitation 2015. Resuscitation. 2015;95:202–222. doi: 10.1016/j.resuscitation.2015.07.018. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
