

Genetic Determinants of Outcome in Intrahepatic Cholangiocarcinoma
- PMID: 33765338
- PMCID: PMC8713028
- DOI: 10.1002/hep.31829
Genetic Determinants of Outcome in Intrahepatic Cholangiocarcinoma
Abstract
Background and aim: Genetic alterations in intrahepatic cholangiocarcinoma (iCCA) are increasingly well characterized, but their impact on outcome and prognosis remains unknown.
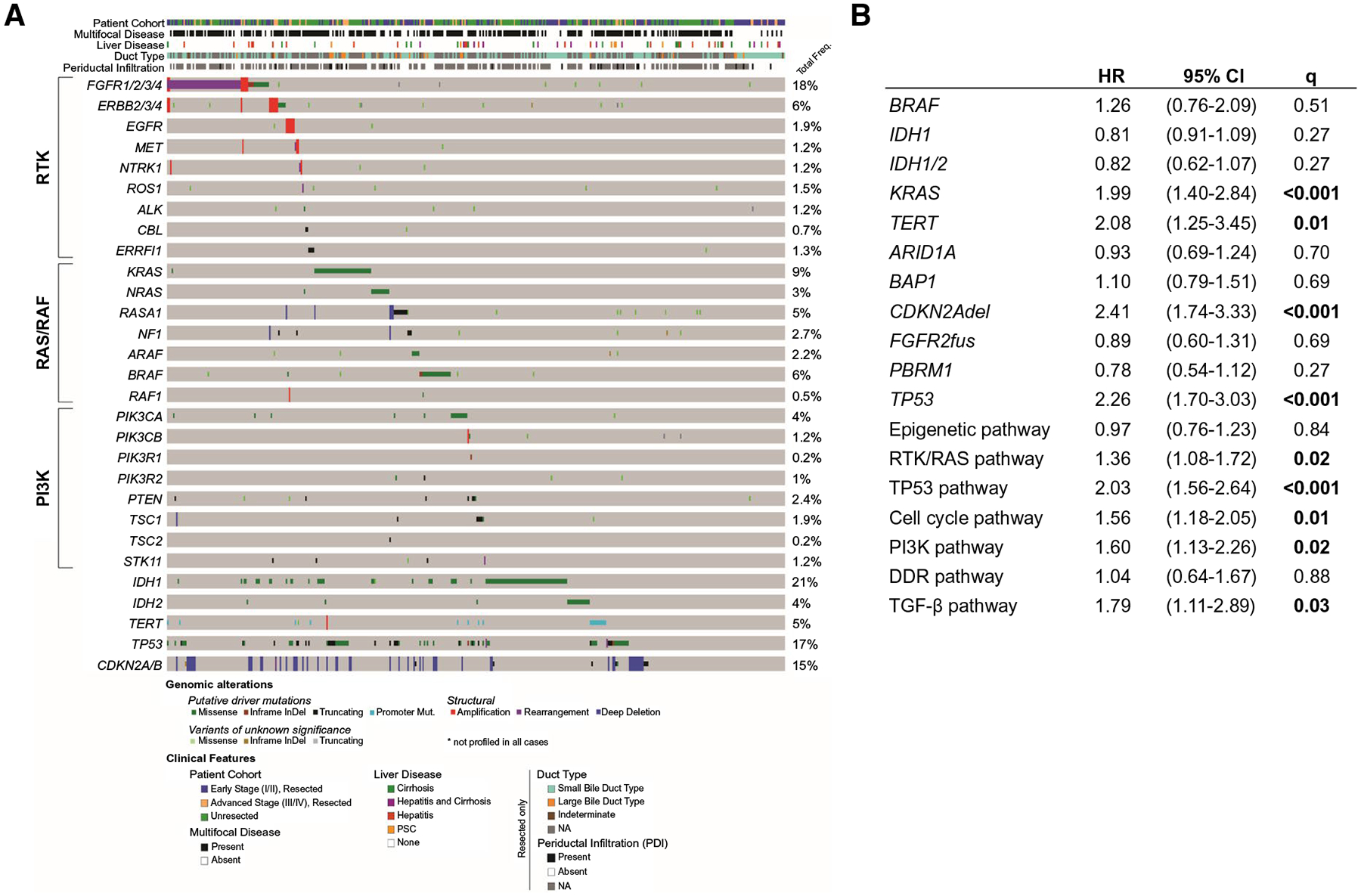
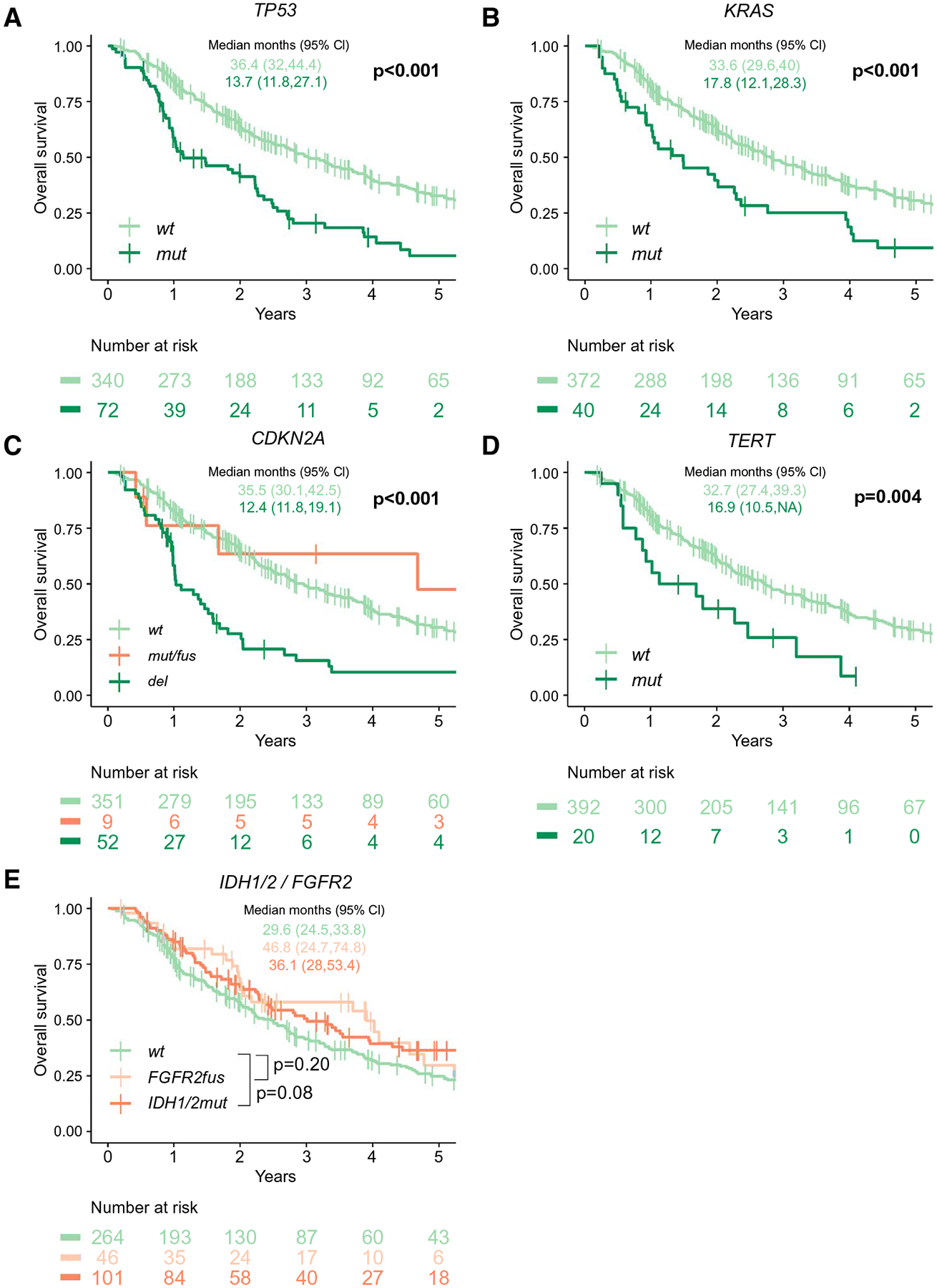
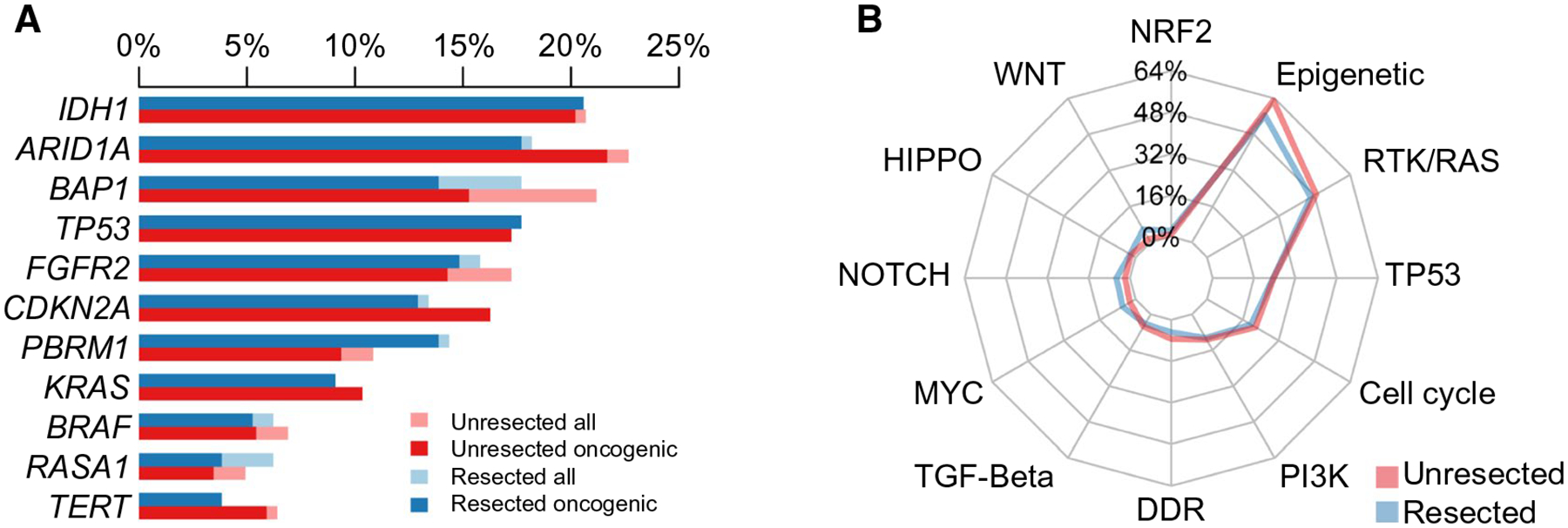
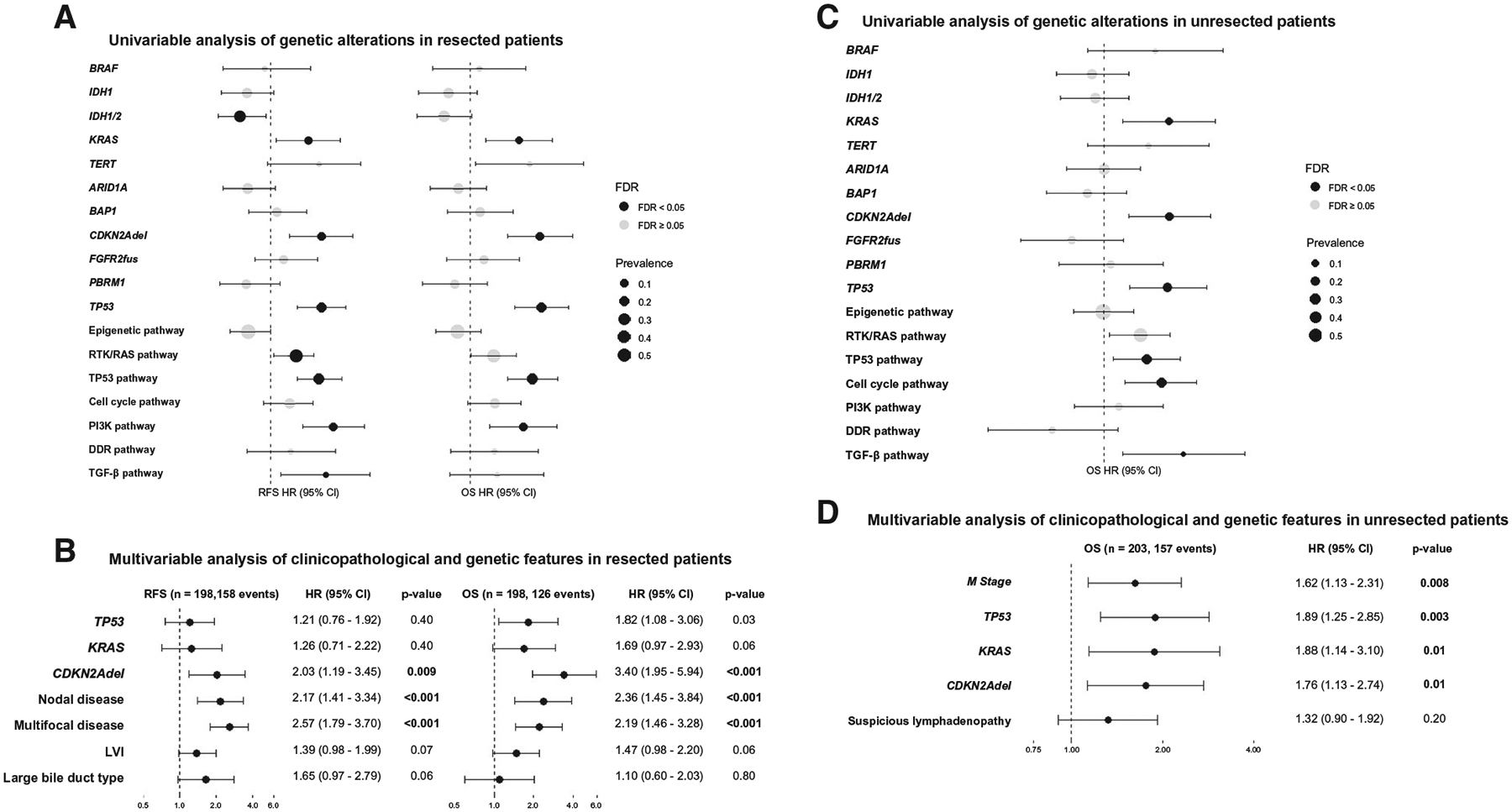
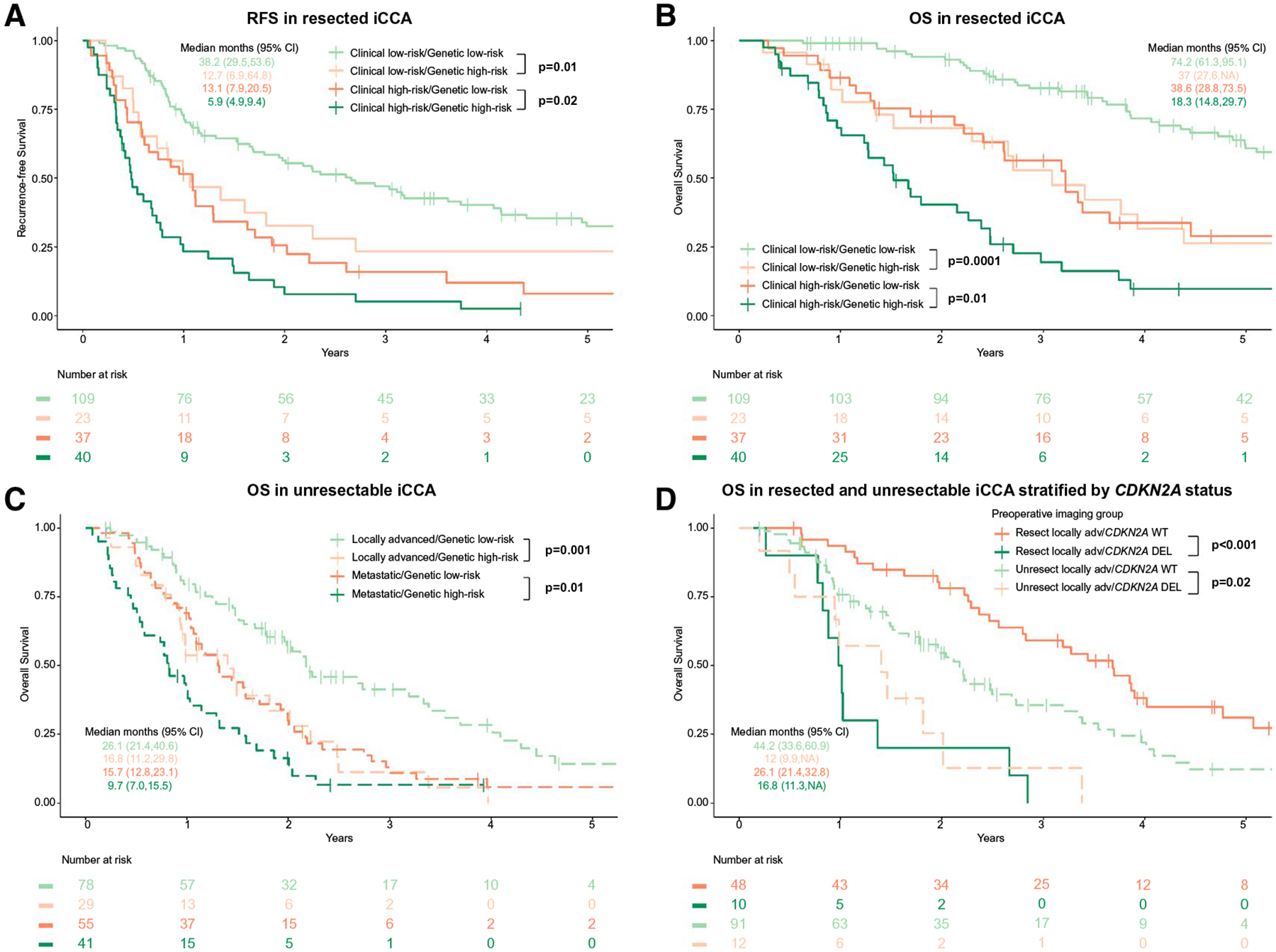
Approach and results: This bi-institutional study of patients with confirmed iCCA (n = 412) used targeted next-generation sequencing of primary tumors to define associations among genetic alterations, clinicopathological variables, and outcome. The most common oncogenic alterations were isocitrate dehydrogenase 1 (IDH1; 20%), AT-rich interactive domain-containing protein 1A (20%), tumor protein P53 (TP53; 17%), cyclin-dependent kinase inhibitor 2A (CDKN2A; 15%), breast cancer 1-associated protein 1 (15%), FGFR2 (15%), polybromo 1 (12%), and KRAS (10%). IDH1/2 mutations (mut) were mutually exclusive with FGFR2 fusions, but neither was associated with outcome. For all patients, TP53 (P < 0.0001), KRAS (P = 0.0001), and CDKN2A (P < 0.0001) alterations predicted worse overall survival (OS). These high-risk alterations were enriched in advanced disease but adversely impacted survival across all stages, even when controlling for known correlates of outcome (multifocal disease, lymph node involvement, bile duct type, periductal infiltration). In resected patients (n = 209), TP53mut (HR, 1.82; 95% CI, 1.08-3.06; P = 0.03) and CDKN2A deletions (del; HR, 3.40; 95% CI, 1.95-5.94; P < 0.001) independently predicted shorter OS, as did high-risk clinical variables (multifocal liver disease [P < 0.001]; regional lymph node metastases [P < 0.001]), whereas KRASmut (HR, 1.69; 95% CI, 0.97-2.93; P = 0.06) trended toward statistical significance. The presence of both or neither high-risk clinical or genetic factors represented outcome extremes (median OS, 18.3 vs. 74.2 months; P < 0.001), with high-risk genetic alterations alone (median OS, 38.6 months; 95% CI, 28.8-73.5) or high-risk clinical variables alone (median OS, 37.0 months; 95% CI, 27.6-not available) associated with intermediate outcome. TP53mut, KRASmut, and CDKN2Adel similarly predicted worse outcome in patients with unresectable iCCA. CDKN2Adel tumors with high-risk clinical features were notable for limited survival and no benefit of resection over chemotherapy.
Conclusions: TP53, KRAS, and CDKN2A alterations were independent prognostic factors in iCCA when controlling for clinical and pathologic variables, disease stage, and treatment. Because genetic profiling can be integrated into pretreatment therapeutic decision-making, combining clinical variables with targeted tumor sequencing may identify patient subgroups with poor outcome irrespective of treatment strategy.
© 2021 by the American Association for the Study of Liver Diseases.
Figures
References
-
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology 2001;33:1353–1357. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
