

Routine asymptomatic testing strategies for airline travel during the COVID-19 pandemic: a simulation study
- PMID: 33765417
- PMCID: PMC7984872
- DOI: 10.1016/S1473-3099(21)00134-1
Routine asymptomatic testing strategies for airline travel during the COVID-19 pandemic: a simulation study
Erratum in
-
Correction to Lancet Infect Dis 2021; 21: 929-38.Lancet Infect Dis. 2021 Dec;21(12):e363. doi: 10.1016/S1473-3099(21)00614-9. Epub 2021 Sep 15. Lancet Infect Dis. 2021. PMID: 34536348 Free PMC article. No abstract available.
Abstract
Background: Routine viral testing strategies for SARS-CoV-2 infection might facilitate safe airline travel during the COVID-19 pandemic and mitigate global spread of the virus. However, the effectiveness of these test-and-travel strategies to reduce passenger risk of SARS-CoV-2 infection and population-level transmission remains unknown.
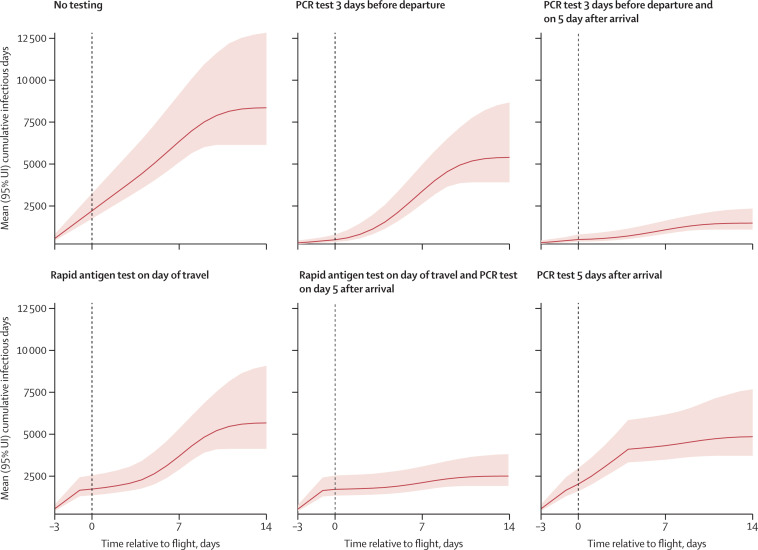
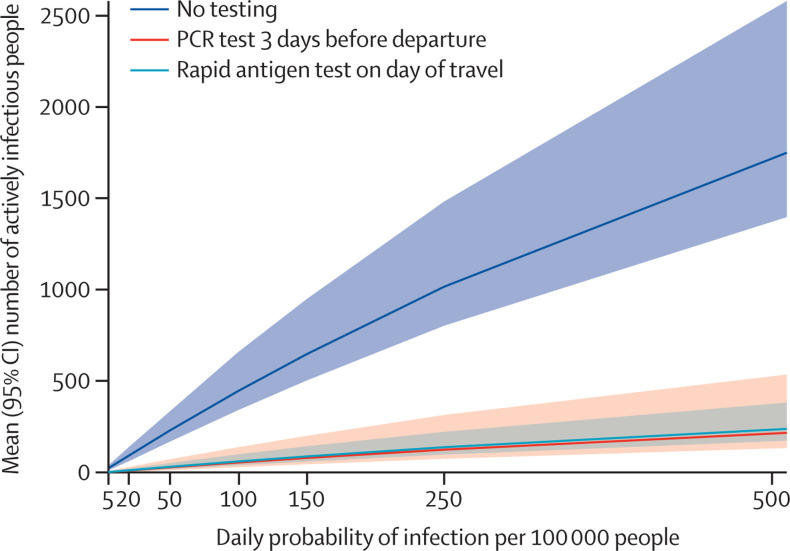
Methods: In this simulation study, we developed a microsimulation of SARS-CoV-2 transmission in a cohort of 100 000 US domestic airline travellers using publicly available data on COVID-19 clinical cases and published natural history parameters to assign individuals one of five health states of susceptible to infection, latent period, early infection, late infection, or recovered. We estimated a per-day risk of infection with SARS-CoV-2 corresponding to a daily incidence of 150 infections per 100 000 people. We assessed five testing strategies: (1) anterior nasal PCR test within 3 days of departure, (2) PCR within 3 days of departure and 5 days after arrival, (3) rapid antigen test on the day of travel (assuming 90% of the sensitivity of PCR during active infection), (4) rapid antigen test on the day of travel and PCR test 5 days after arrival, and (5) PCR test 5 days after arrival. Strategies 2 and 4 included a 5-day quarantine after arrival. The travel period was defined as 3 days before travel to 2 weeks after travel. Under each scenario, individuals who tested positive before travel were not permitted to travel. The primary study outcome was cumulative number of infectious days in the cohort over the travel period without isolation or quarantine (population-level transmission risk), and the key secondary outcome was the number of infectious people detected on the day of travel (passenger risk of infection).
Findings: We estimated that in a cohort of 100 000 airline travellers, in a scenario with no testing or screening, there would be 8357 (95% uncertainty interval 6144-12831) infectious days with 649 (505-950) actively infectious passengers on the day of travel. The pre-travel PCR test reduced the number of infectious days from 8357 to 5401 (3917-8677), a reduction of 36% (29-41) compared with the base case, and identified 569 (88% [76-92]) of 649 actively infectious travellers on the day of flight; the addition of post-travel quarantine and PCR reduced the number of infectious days to 2520 days (1849-4158), a reduction of 70% (64-75) compared with the base case. The rapid antigen test on the day of travel reduced the number of infectious days to 5674 (4126-9081), a reduction of 32% (26-38) compared with the base case, and identified 560 (86% [83-89]) actively infectious travellers; the addition of post-travel quarantine and PCR reduced the number of infectious days to 3124 (2356-495), a reduction of 63% (58-66) compared with the base case. The post-travel PCR alone reduced the number of infectious days to 4851 (3714-7679), a reduction of 42% (35-49) compared with the base case.
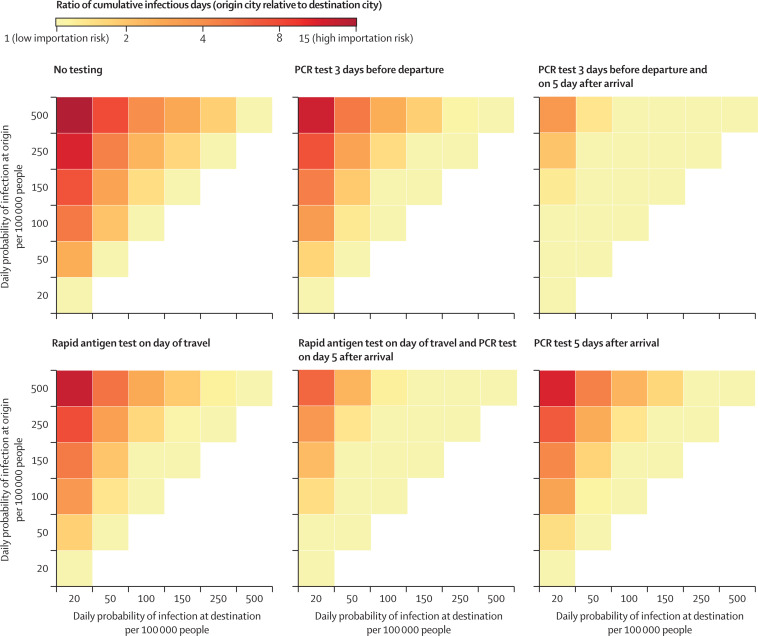
Interpretation: Routine asymptomatic testing for SARS-CoV-2 before travel can be an effective strategy to reduce passenger risk of infection during travel, although abbreviated quarantine with post-travel testing is probably needed to reduce population-level transmission due to importation of infection when travelling from a high to low incidence setting.
Funding: University of California, San Francisco.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
Update of
-
Routine asymptomatic testing strategies for airline travel during the COVID-19 pandemic: a simulation analysis.medRxiv [Preprint]. 2020 Dec 11:2020.12.08.20246132. doi: 10.1101/2020.12.08.20246132. medRxiv. 2020. Update in: Lancet Infect Dis. 2021 Jul;21(7):929-938. doi: 10.1016/S1473-3099(21)00134-1. PMID: 33330886 Free PMC article. Updated. Preprint.
Comment in
-
Two-test or three-test strategy for routine asymptomatic testing during air travel?Lancet Infect Dis. 2021 Sep;21(9):1214-1215. doi: 10.1016/S1473-3099(21)00357-1. Epub 2021 Jun 28. Lancet Infect Dis. 2021. PMID: 34197766 Free PMC article. No abstract available.
-
Addendum needed on COVID-19 travel study.Lancet Infect Dis. 2021 Nov;21(11):1494-1495. doi: 10.1016/S1473-3099(21)00454-0. Epub 2021 Sep 15. Lancet Infect Dis. 2021. PMID: 34536350 Free PMC article. No abstract available.
-
Addendum needed on COVID-19 travel study - Authors' reply.Lancet Infect Dis. 2021 Nov;21(11):1495-1496. doi: 10.1016/S1473-3099(21)00562-4. Epub 2021 Sep 15. Lancet Infect Dis. 2021. PMID: 34536351 Free PMC article. No abstract available.
Similar articles
-
Routine asymptomatic testing strategies for airline travel during the COVID-19 pandemic: a simulation analysis.medRxiv [Preprint]. 2020 Dec 11:2020.12.08.20246132. doi: 10.1101/2020.12.08.20246132. medRxiv. 2020. Update in: Lancet Infect Dis. 2021 Jul;21(7):929-938. doi: 10.1016/S1473-3099(21)00134-1. PMID: 33330886 Free PMC article. Updated. Preprint.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
International travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2021 Mar 25;3(3):CD013717. doi: 10.1002/14651858.CD013717.pub2. Cochrane Database Syst Rev. 2021. PMID: 33763851 Free PMC article.
-
Travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2020 Oct 5;10:CD013717. doi: 10.1002/14651858.CD013717. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 25;3:CD013717. doi: 10.1002/14651858.CD013717.pub2. PMID: 33502002 Updated.
-
Strategies to reduce the risk of SARS-CoV-2 importation from international travellers: modelling estimations for the United Kingdom, July 2020.Euro Surveill. 2021 Sep;26(39):2001440. doi: 10.2807/1560-7917.ES.2021.26.39.2001440. Euro Surveill. 2021. PMID: 34596018 Free PMC article.
Cited by
-
SARS-CoV-2 screening strategies for returning international travellers: Evaluation of a rapid antigen test approach.Int J Infect Dis. 2022 May;118:126-131. doi: 10.1016/j.ijid.2022.02.045. Epub 2022 Mar 2. Int J Infect Dis. 2022. PMID: 35247549 Free PMC article.
-
Performance of Three Tests for SARS-CoV-2 on a University Campus Estimated Jointly with Bayesian Latent Class Modeling.Microbiol Spectr. 2022 Feb 23;10(1):e0122021. doi: 10.1128/spectrum.01220-21. Epub 2022 Jan 19. Microbiol Spectr. 2022. PMID: 35044220 Free PMC article.
-
Two-test or three-test strategy for routine asymptomatic testing during air travel?Lancet Infect Dis. 2021 Sep;21(9):1214-1215. doi: 10.1016/S1473-3099(21)00357-1. Epub 2021 Jun 28. Lancet Infect Dis. 2021. PMID: 34197766 Free PMC article. No abstract available.
-
Correlation between notifiable infectious diseases and transportation passenger traffic from 2013 to 2019 in mainland China.BMC Public Health. 2024 Oct 31;24(1):3023. doi: 10.1186/s12889-024-20479-9. BMC Public Health. 2024. PMID: 39482638 Free PMC article.
-
Framework for assessing and easing global COVID-19 travel restrictions.Sci Rep. 2022 Apr 28;12(1):6985. doi: 10.1038/s41598-022-10678-y. Sci Rep. 2022. PMID: 35484268 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
