

Longitudinal profiling of respiratory and systemic immune responses reveals myeloid cell-driven lung inflammation in severe COVID-19
- PMID: 33765436
- PMCID: PMC7951561
- DOI: 10.1016/j.immuni.2021.03.005
Longitudinal profiling of respiratory and systemic immune responses reveals myeloid cell-driven lung inflammation in severe COVID-19
Abstract
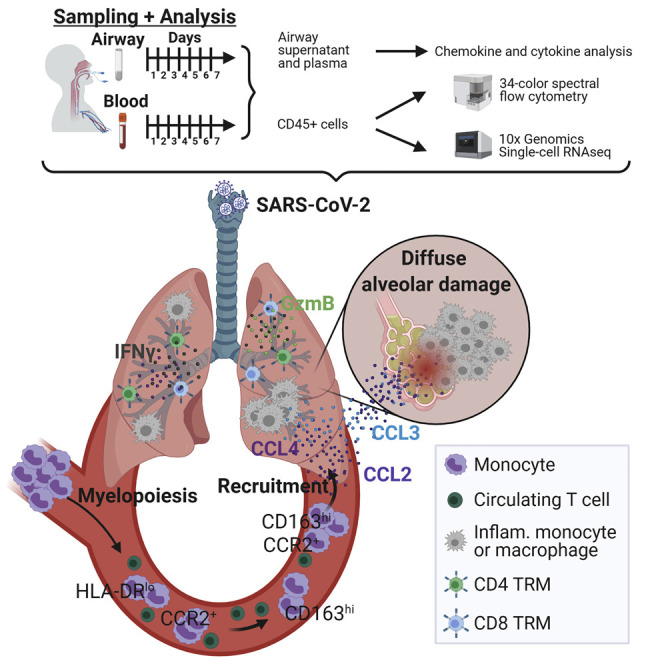
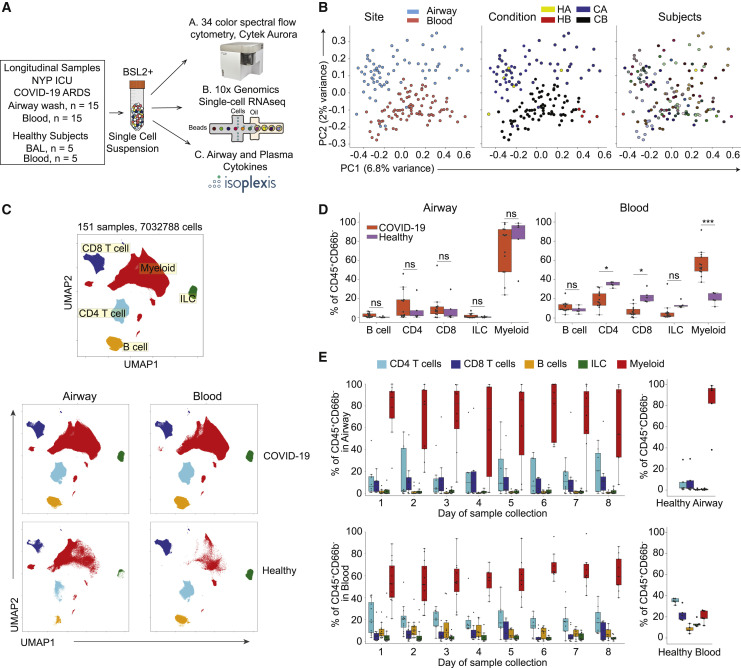
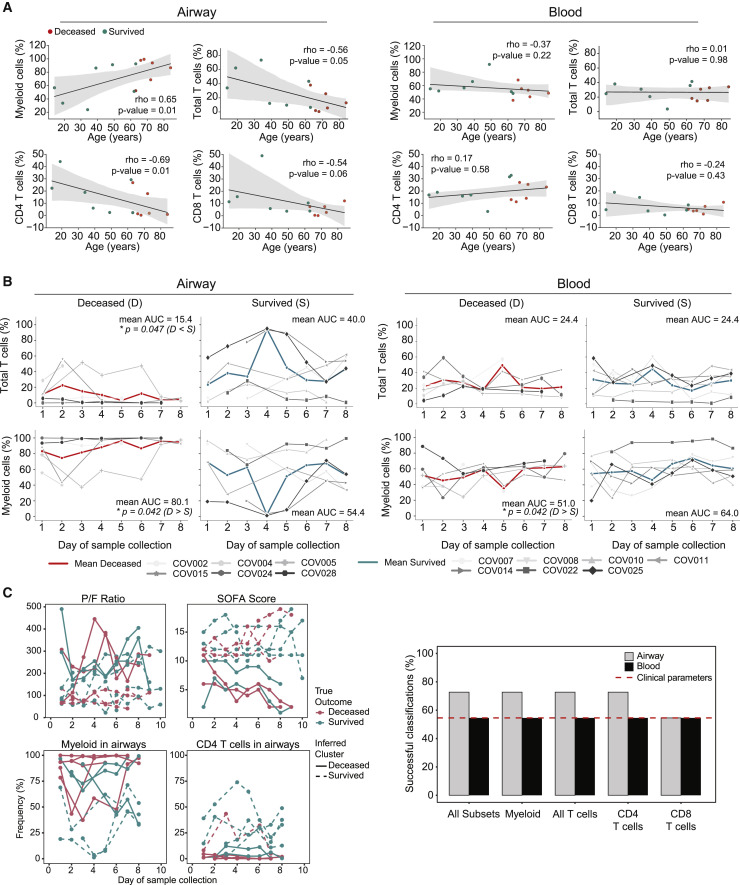
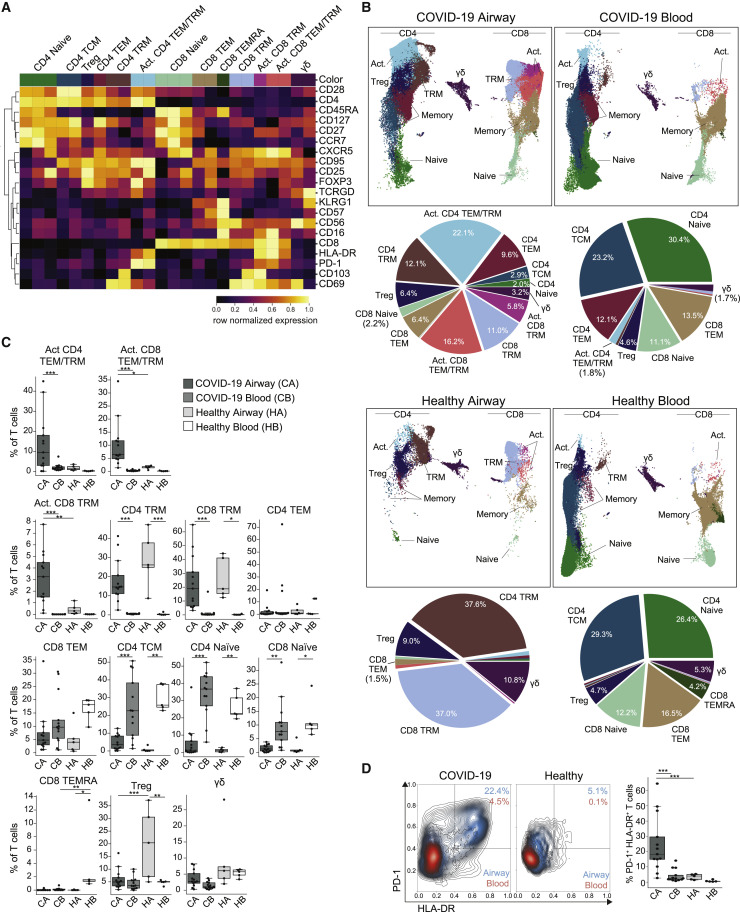
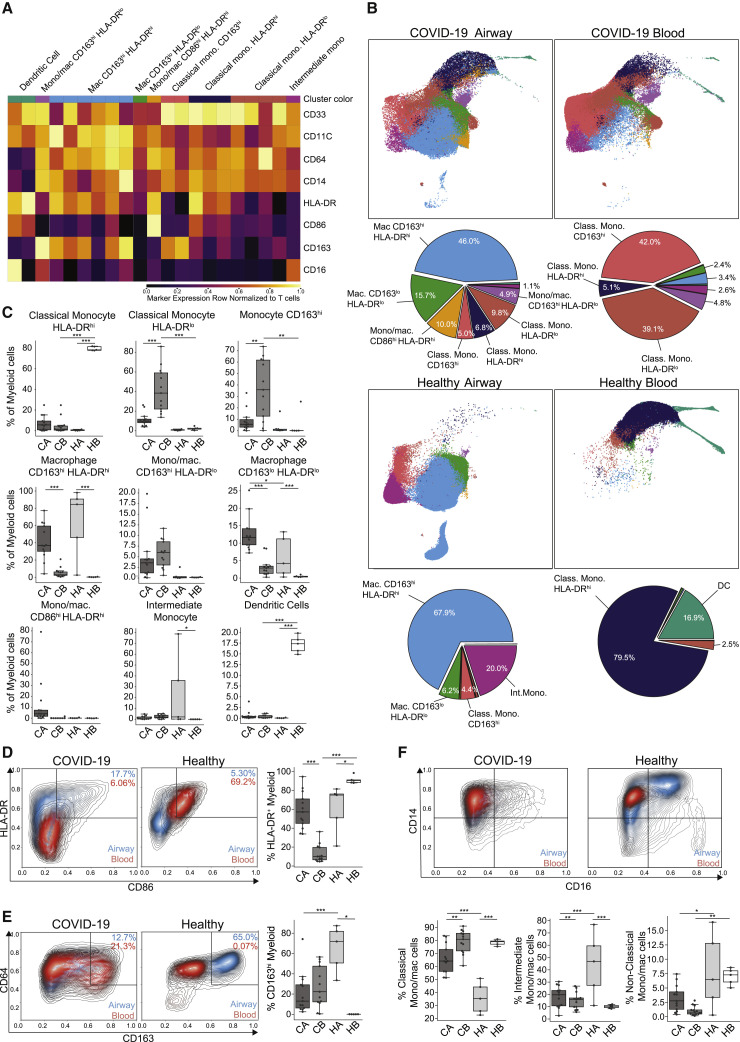
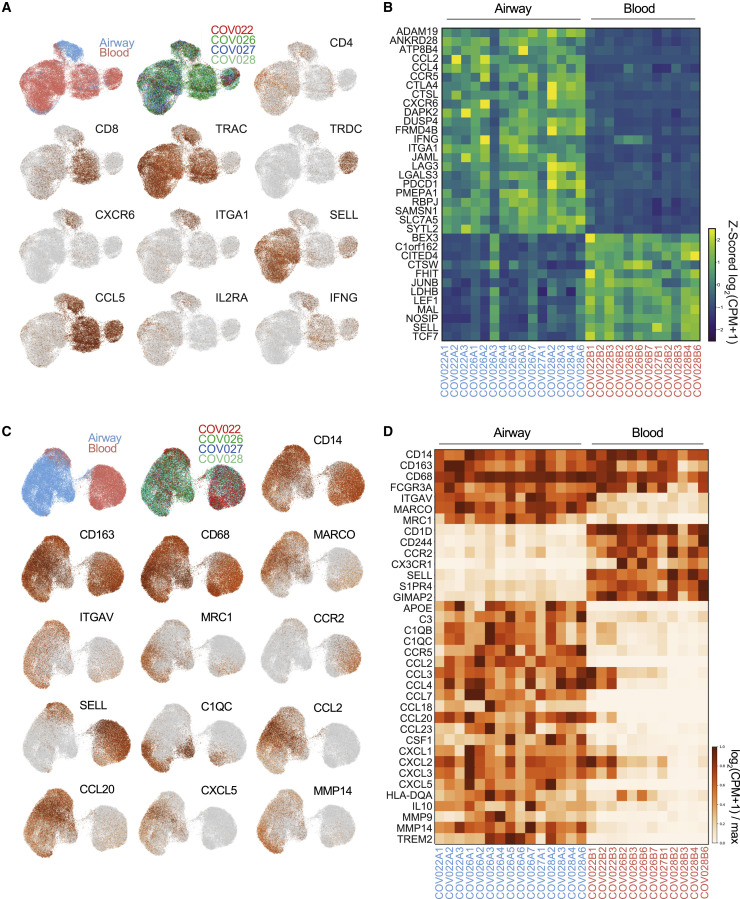
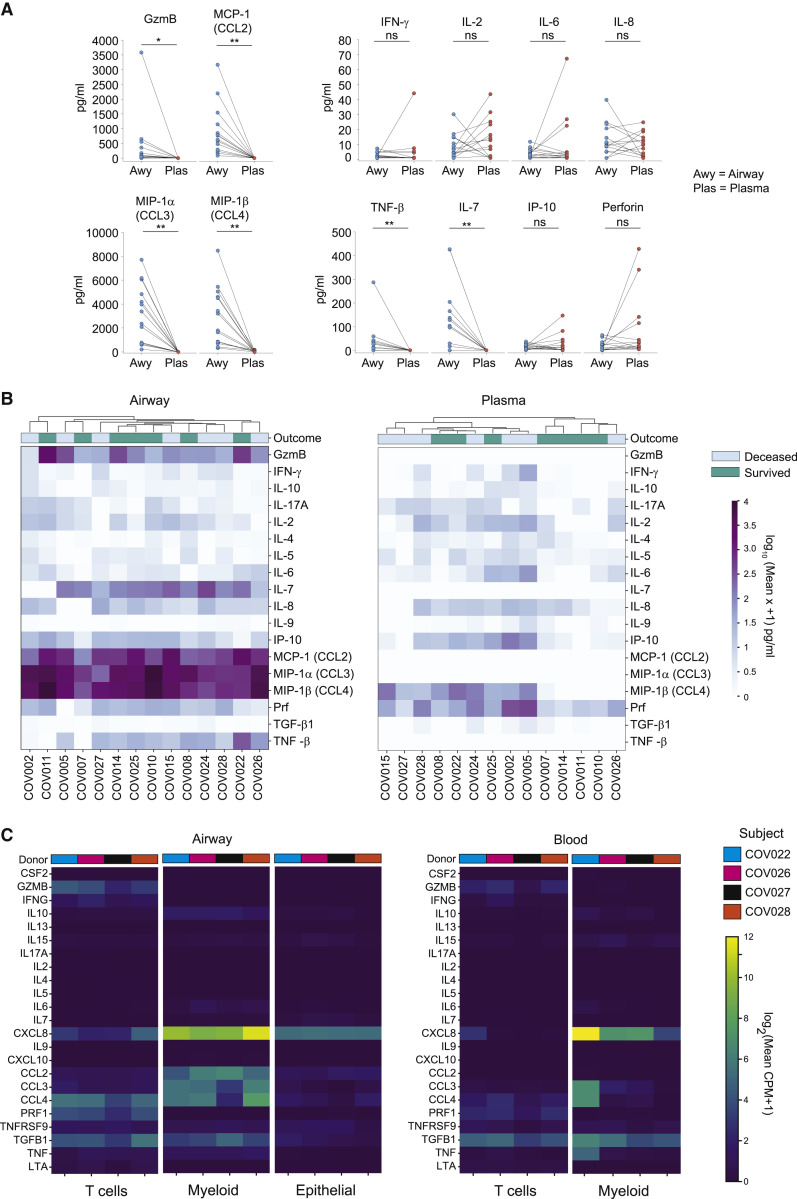
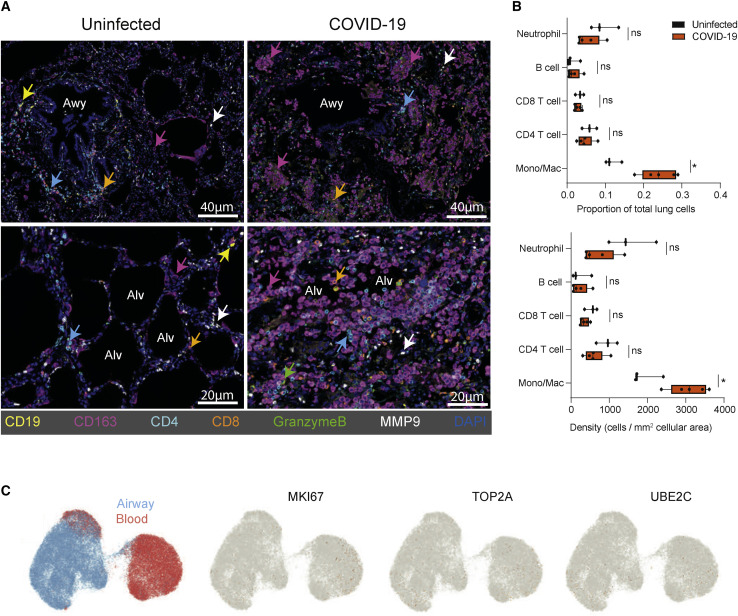
Immune response dynamics in coronavirus disease 2019 (COVID-19) and their severe manifestations have largely been studied in circulation. Here, we examined the relationship between immune processes in the respiratory tract and circulation through longitudinal phenotypic, transcriptomic, and cytokine profiling of paired airway and blood samples from patients with severe COVID-19 relative to heathy controls. In COVID-19 airways, T cells exhibited activated, tissue-resident, and protective profiles; higher T cell frequencies correlated with survival and younger age. Myeloid cells in COVID-19 airways featured hyperinflammatory signatures, and higher frequencies of these cells correlated with mortality and older age. In COVID-19 blood, aberrant CD163+ monocytes predominated over conventional monocytes, and were found in corresponding airway samples and in damaged alveoli. High levels of myeloid chemoattractants in airways suggest recruitment of these cells through a CCL2-CCR2 chemokine axis. Our findings provide insights into immune processes driving COVID-19 lung pathology with therapeutic implications for targeting inflammation in the respiratory tract.
Keywords: ARDS; COVID-19; chemokines; coronavirus disease 2019; cytokines; lung immunity; macrophages; monocytes; single-cell RNA sequencing; tissue resident memory T cells.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests J.Z., M.S., and S.M. have competing interests with IsoPlexis. The remaining authors declare no competing interests.
Figures
Update of
-
Analysis of respiratory and systemic immune responses in COVID-19 reveals mechanisms of disease pathogenesis.medRxiv [Preprint]. 2020 Oct 18:2020.10.15.20208041. doi: 10.1101/2020.10.15.20208041. medRxiv. 2020. Update in: Immunity. 2021 Apr 13;54(4):797-814.e6. doi: 10.1016/j.immuni.2021.03.005. PMID: 33106817 Free PMC article. Updated. Preprint.
Comment in
-
Monocytes and macrophages in severe COVID-19 - friend, foe or both?Immunol Cell Biol. 2021 Jul;99(6):561-564. doi: 10.1111/imcb.12464. Epub 2021 May 30. Immunol Cell Biol. 2021. PMID: 34053124 Free PMC article. No abstract available.
References
-
- Bharat A., Bhorade S.M., Morales-Nebreda L., McQuattie-Pimentel A.C., Soberanes S., Ridge K., DeCamp M.M., Mestan K.K., Perlman H., Budinger G.R., Misharin A.V. Flow Cytometry Reveals Similarities Between Lung Macrophages in Humans and Mice. Am. J. Respir. Cell Mol. Biol. 2016;54:147–149. - PMC - PubMed
-
- Bray N.L., Pimentel H., Melsted P., Pachter L. Near-optimal probabilistic RNA-seq quantification. Nat. Biotechnol. 2016;34:525–527. - PubMed
-
- Carpenter D.J., Granot T., Matsuoka N., Senda T., Kumar B.V., Thome J.J.C., Gordon C.L., Miron M., Weiner J., Connors T., et al. Human immunology studies using organ donors: impact of clinical variations on immune parameters in tissues and circulation. Am. J. Transplant. 2018;18:74–88. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
