

Incidence and prevalence of tuberculosis in incarcerated populations: a systematic review and meta-analysis
- PMID: 33765455
- PMCID: PMC8168455
- DOI: 10.1016/S2468-2667(21)00025-6
Incidence and prevalence of tuberculosis in incarcerated populations: a systematic review and meta-analysis
Abstract
Background: Prisons are recognised as high-risk environments for tuberculosis, but there has been little systematic investigation of the global and regional incidence and prevalence of tuberculosis, and its determinants, in prisons. We did a systematic review and meta-analysis to assess the incidence and prevalence of tuberculosis in incarcerated populations by geographical region.
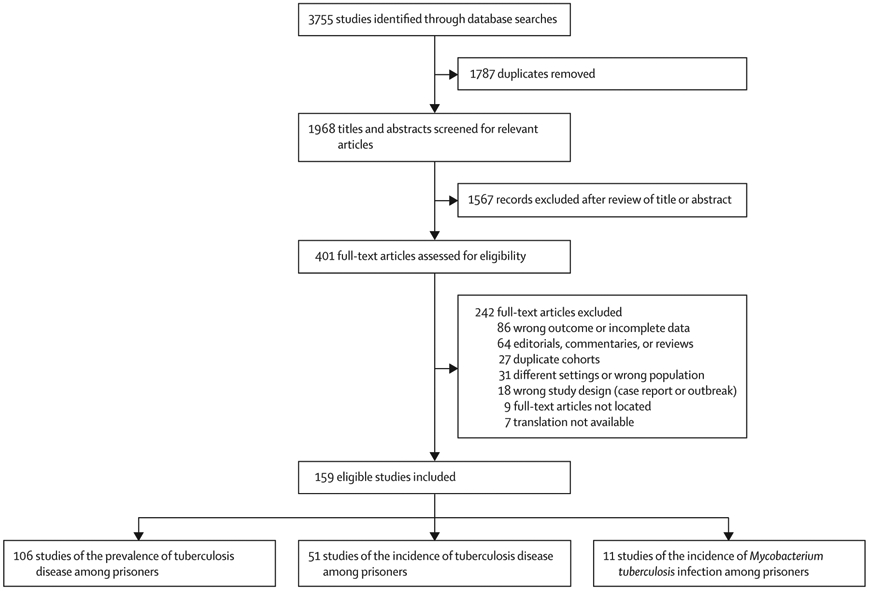
Methods: In this systematic review and meta-analysis, we searched MEDLINE, Embase, Web of Knowledge, and the LILACS electronic database from Jan 1, 1980, to Nov 15, 2020, for cross-sectional and cohort studies reporting the incidence of Mycobacterium tuberculosis infection, incidence of tuberculosis, or prevalence of tuberculosis among incarcerated individuals in all geographical regions. We extracted data from individual studies, and calculated pooled estimates of incidence and prevalence through hierarchical Bayesian meta-regression modelling. We also did subgroup analyses by region. Incidence rate ratios between prisons and the general population were calculated by dividing the incidence of tuberculosis in prisons by WHO estimates of the national population-level incidence.
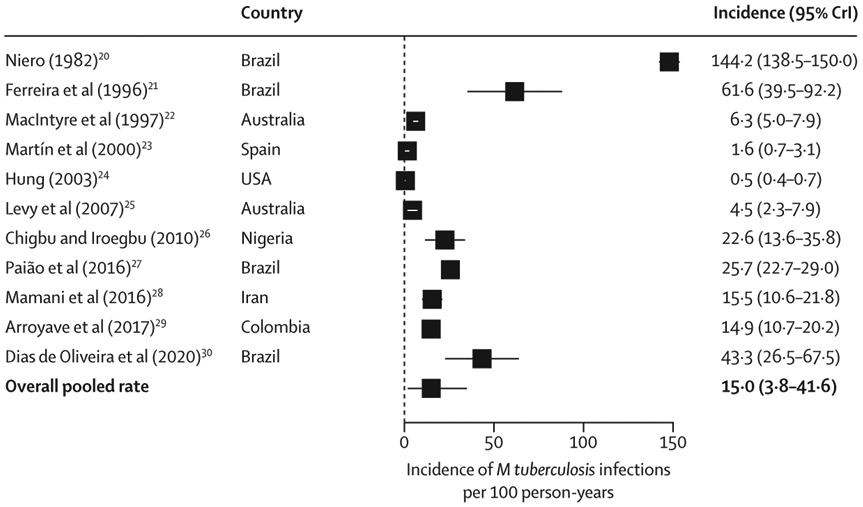
Findings: We identified 159 relevant studies; 11 investigated the incidence of M tuberculosis infection (n=16 318), 51 investigated the incidence of tuberculosis (n=1 858 323), and 106 investigated the prevalence of tuberculosis (n=6 727 513) in incarcerated populations. The overall pooled incidence of M tuberculosis infection among prisoners was 15·0 (95% credible interval [CrI] 3·8-41·6) per 100 person-years. The incidence of tuberculosis (per 100 000 person-years) among prisoners was highest in studies from the WHO African (2190 [95% CrI 810-4840] cases) and South-East Asia (1550 [240-5300] cases) regions and in South America (970 [460-1860] cases), and lowest in North America (30 [20-50] cases) and the WHO Eastern Mediterranean region (270 [50-880] cases). The prevalence of tuberculosis was greater than 1000 per 100 000 prisoners in all global regions except for North America and the Western Pacific, and highest in the WHO South-East Asia region (1810 [95% CrI 670-4000] cases per 100 000 prisoners). The incidence rate ratio between prisons and the general population was much higher in South America (26·9; 95% CrI 17·1-40·1) than in other regions, but was nevertheless higher than ten in the WHO African (12·6; 6·2-22·3), Eastern Mediterranean (15·6; 6·5-32·5), and South-East Asia (11·7; 4·1-27·1) regions.
Interpretation: Globally, people in prison are at high risk of contracting M tuberculosis infection and developing tuberculosis, with consistent disparities between prisons and the general population across regions. Tuberculosis control programmes should prioritise preventive interventions among incarcerated populations.
Funding: US National Institutes of Health.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
Tuberculosis in prisons: an unintended sentence?Lancet Public Health. 2021 May;6(5):e263-e264. doi: 10.1016/S2468-2667(21)00049-9. Epub 2021 Mar 22. Lancet Public Health. 2021. PMID: 33765454 No abstract available.
References
-
- WHO. Global tuberculosis report 2020. Geneva: World Health Organization, 2020.
-
- WHO. Latent tuberculosis infection: updated and consolidated guidelines for programmatic management (WHO/CDS/TB/2018.4). Geneva: World Health Organization, 2018. - PubMed
-
- Walmsley R. World prison population list. London: Institute for Criminal Policy Research, 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
