

Birthweight: EN-BIRTH multi-country validation study
- PMID: 33765936
- PMCID: PMC7995711
- DOI: 10.1186/s12884-020-03355-3
Birthweight: EN-BIRTH multi-country validation study
Abstract
Background: Accurate birthweight is critical to inform clinical care at the individual level and tracking progress towards national/global targets at the population level. Low birthweight (LBW) < 2500 g affects over 20.5 million newborns annually. However, data are lacking and may be affected by heaping. This paper evaluates birthweight measurement within the Every Newborn Birth Indicators Research Tracking in Hospitals (EN-BIRTH) study.
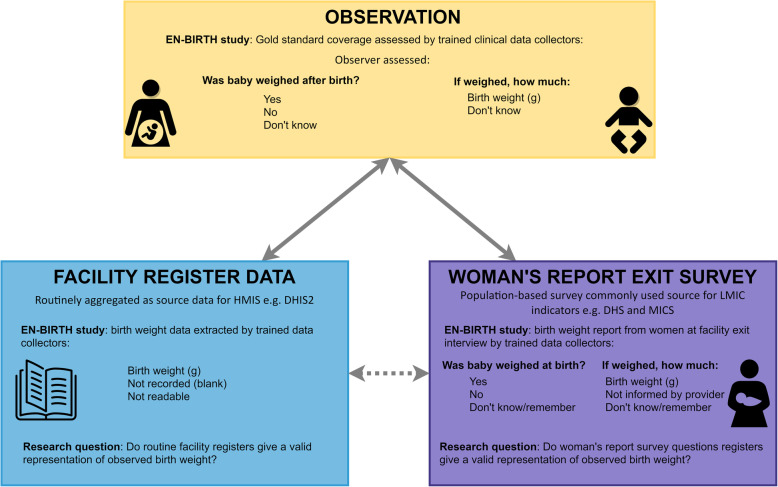
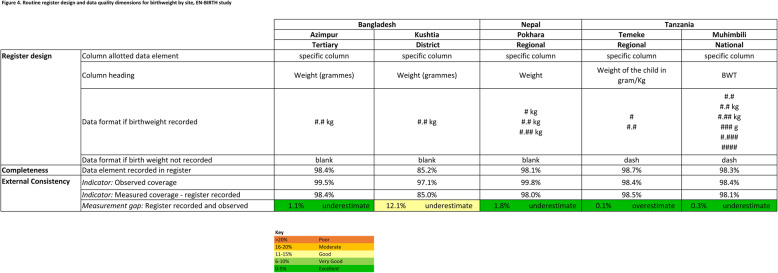
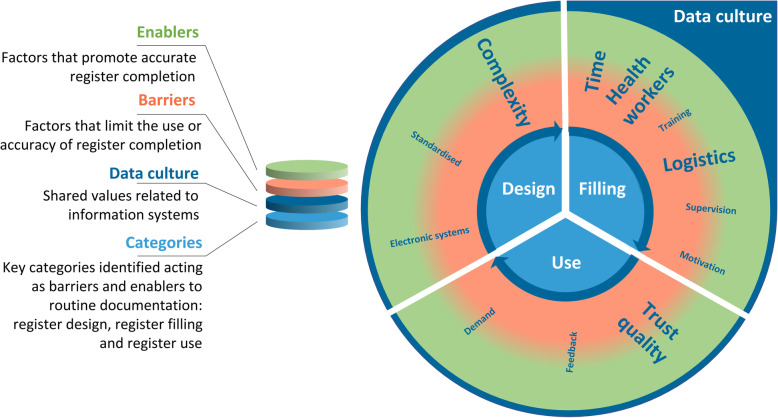
Methods: The EN-BIRTH study took place in five hospitals in Bangladesh, Nepal and Tanzania (2017-2018). Clinical observers collected time-stamped data (gold standard) for weighing at birth. We compared accuracy for two data sources: routine hospital registers and women's report at exit interview survey. We calculated absolute differences and individual-level validation metrics. We analysed birthweight coverage and quality gaps including timing and heaping. Qualitative data explored barriers and enablers for routine register data recording.
Results: Among 23,471 observed births, 98.8% were weighed. Exit interview survey-reported weighing coverage was 94.3% (90.2-97.3%), sensitivity 95.0% (91.3-97.8%). Register-reported coverage was 96.6% (93.2-98.9%), sensitivity 97.1% (94.3-99%). Routine registers were complete (> 98% for four hospitals) and legible > 99.9%. Weighing of stillbirths varied by hospital, ranging from 12.5-89.0%. Observed LBW rate was 15.6%; survey-reported rate 14.3% (8.9-20.9%), sensitivity 82.9% (75.1-89.4%), specificity 96.1% (93.5-98.5%); register-recorded rate 14.9%, sensitivity 90.8% (85.9-94.8%), specificity 98.5% (98-99.0%). In surveys, "don't know" responses for birthweight measured were 4.7%, and 2.9% for knowing the actual weight. 95.9% of observed babies were weighed within 1 h of birth, only 14.7% with a digital scale. Weight heaping indices were around two-fold lower using digital scales compared to analogue. Observed heaping was almost 5% higher for births during the night than day. Survey-report further increased observed birthweight heaping, especially for LBW babies. Enablers to register birthweight measurement in qualitative interviews included digital scale availability and adequate staffing.
Conclusions: Hospital registers captured birthweight and LBW prevalence more accurately than women's survey report. Even in large hospitals, digital scales were not always available and stillborn babies not always weighed. Birthweight data are being captured in hospitals and investment is required to further improve data quality, researching of data flow in routine systems and use of data at every level.
Keywords: Birth; Birthweight; Coverage; Health management information systems; Low birthweight; Maternal; Newborn; Stillbirth; Survey; Validity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- World Health Organization: Reproductive Health Indicators: Guidelines for Their Generation, Interpretation, and Analysis for Global Monitoring. https://www.who.int/reproductivehealth/publications/monitoring/924156315.... Accessed 14 Aug 2020.
-
- World Health Organization: Global Targets 2025. https://www.who.int/nutrition/global-target-2025/en/]. Accessed 9 Dec 2019.
-
- UNICEF, WHO: UNICEF-WHO low birthweight estimates: levels and trends 2000–2015. https://www.unicef.org/reports/UNICEF-WHO-low-birthweight-estimates-2019/. Accessed 14 Aug 2020.
-
- World Health Organization: Survive and Thrive: Transforming Care for Every Small and Sick Newborn. https://www.unicef.org/reports/transforming-care-for-every-small-and-sic.... Accessed 13 Aug 2020.
-
- Blencowe H, Krasevec J, de Onis M, Black RE, An X, Stevens GA, Borghi E, Hayashi C, Estevez D, Cegolon L, et al. National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health. 2019;7(7):e849–e860. doi: 10.1016/S2214-109X(18)30565-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
