

Immediate newborn care and breastfeeding: EN-BIRTH multi-country validation study
- PMID: 33765946
- PMCID: PMC7995709
- DOI: 10.1186/s12884-020-03421-w
Immediate newborn care and breastfeeding: EN-BIRTH multi-country validation study
Abstract
Background: Immediate newborn care (INC) practices, notably early initiation of breastfeeding (EIBF), are fundamental for newborn health. However, coverage tracking currently relies on household survey data in many settings. "Every Newborn Birth Indicators Research Tracking in Hospitals" (EN-BIRTH) was an observational study validating selected maternal and newborn health indicators. This paper reports results for EIBF.
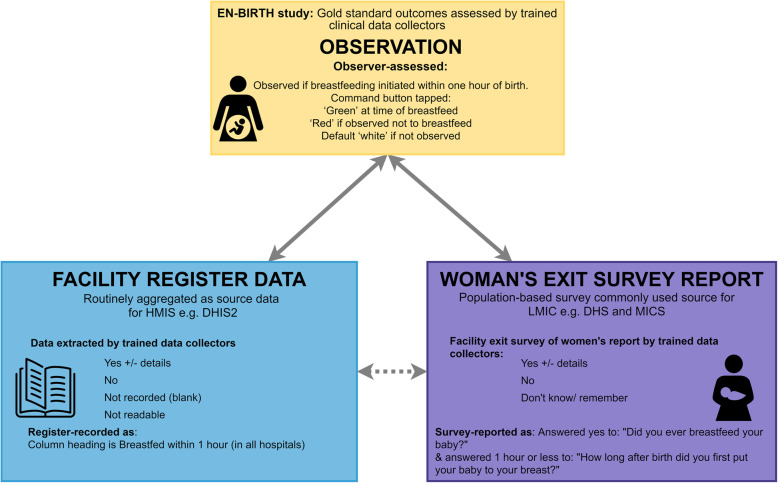
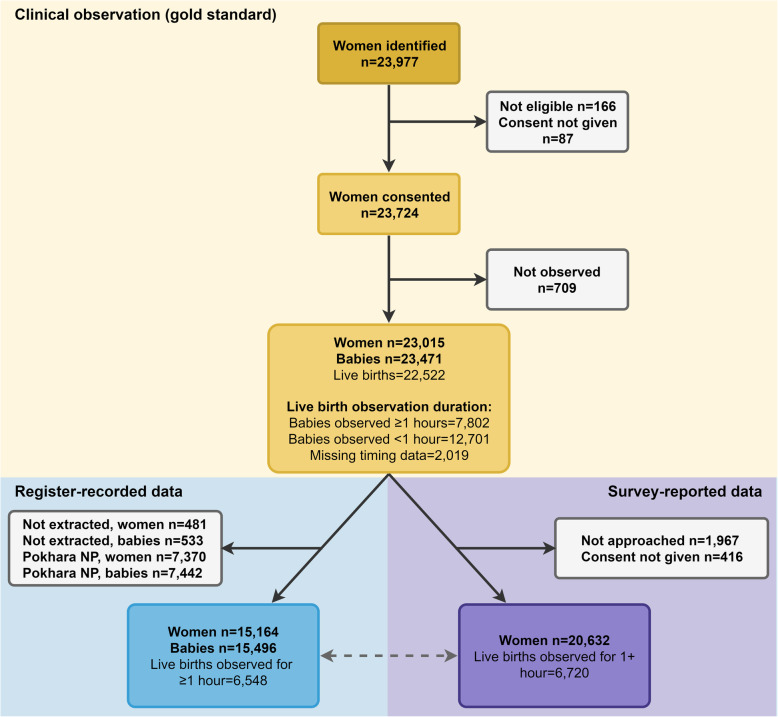
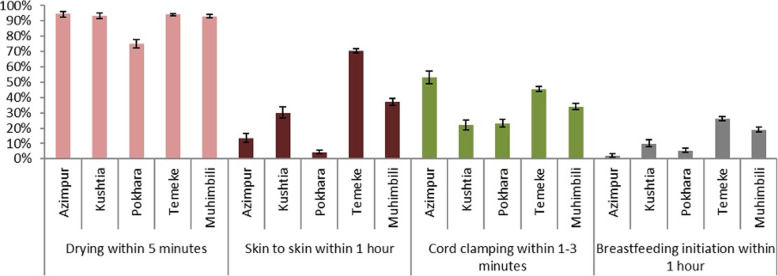
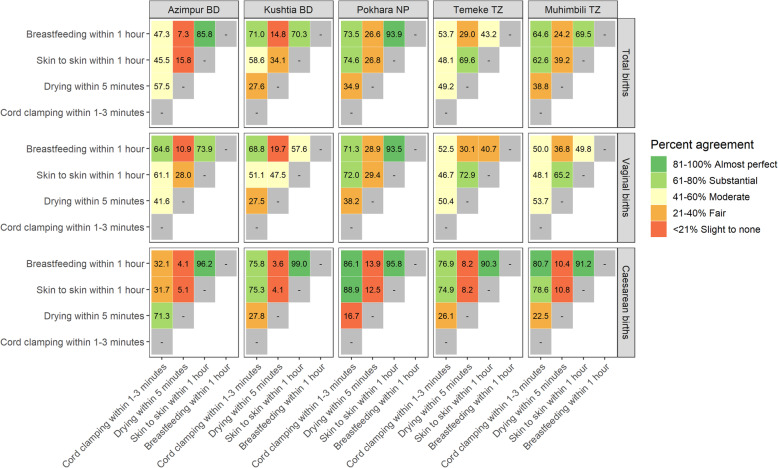
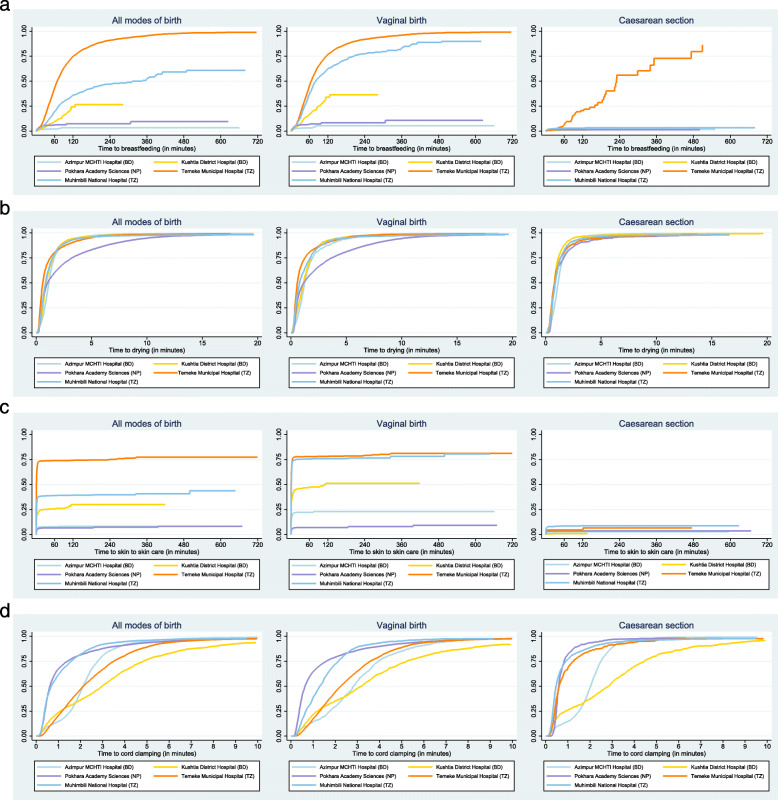
Methods: The EN-BIRTH study was conducted in five public hospitals in Bangladesh, Nepal, and Tanzania, from July 2017 to July 2018. Clinical observers collected tablet-based, time-stamped data on EIBF and INC practices (skin-to-skin within 1 h of birth, drying, and delayed cord clamping). To assess validity of EIBF measurement, we compared observation as gold standard to register records and women's exit-interview survey reports. Percent agreement was used to assess agreement between EIBF and INC practices. Kaplan Meier survival curves showed timing. Qualitative interviews were conducted to explore barriers/enablers to register recording.
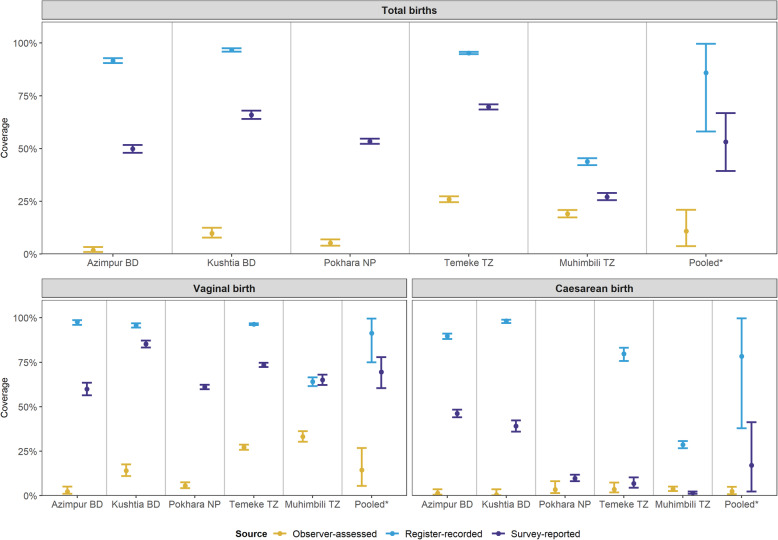
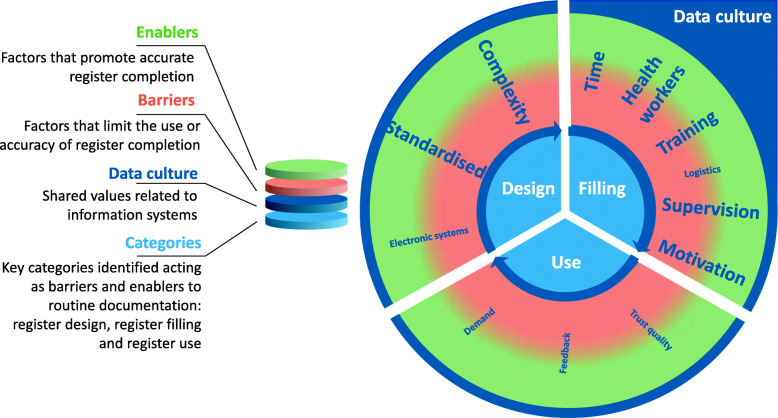
Results: Coverage of EIBF among 7802 newborns observed for ≥1 h was low (10.9, 95% CI 3.8-21.0). Survey-reported (53.2, 95% CI 39.4-66.8) and register-recorded results (85.9, 95% CI 58.1-99.6) overestimated coverage compared to observed levels across all hospitals. Registers did not capture other INC practices apart from breastfeeding. Agreement of EIBF with other INC practices was high for skin-to-skin (69.5-93.9%) at four sites, but fair/poor for delayed cord-clamping (47.3-73.5%) and drying (7.3-29.0%). EIBF and skin-to-skin were the most delayed and EIBF rarely happened after caesarean section (0.5-3.6%). Qualitative findings suggested that focusing on accuracy, as well as completeness, contributes to higher quality with register reporting.
Conclusions: Our study highlights the importance of tracking EIBF despite measurement challenges and found low coverage levels, particularly after caesarean births. Both survey-reported and register-recorded data over-estimated coverage. EIBF had a strong agreement with skin-to-skin but is not a simple tracer for other INC indicators. Other INC practices are challenging to measure in surveys, not included in registers, and are likely to require special studies or audits. Continued focus on EIBF is crucial to inform efforts to improve provider practices and increase coverage. Investment and innovation are required to improve measurement.
Keywords: Birth; Breastfeeding; Health management systems; Hospital records; Immediate newborn care; Maternal; Newborn; Skin-to-skin; Survey; Validity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- United Nations Children’s Fund, World Health Organization, World Bank Group, United Nations DoEaSA, Population Division,, United Nations Economic Commission for Latin America and the Caribbean PD: Levels & Trends in Child Mortality Report 2020. https://www.unicef.org/reports/levels-and-trends-child-mortality-report-.... Accessed 4 Nov 2020.
-
- Hug L, Sharrow, D & You, D. : levels and trends in child mortality: report 2019. Accessed.
-
- World Health Organization: WHO recommendations on newborn health: guidelines approved by the WHO Guidelines Review Committee. Geneva; 2017. https://apps.who.int/iris/handle/10665/259269. Accessed 4 Nov 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
