

Kangaroo mother care: EN-BIRTH multi-country validation study
- PMID: 33765950
- PMCID: PMC7995571
- DOI: 10.1186/s12884-020-03423-8
Kangaroo mother care: EN-BIRTH multi-country validation study
Abstract
Background: Kangaroo mother care (KMC) reduces mortality among stable neonates ≤2000 g. Lack of data tracking coverage and quality of KMC in both surveys and routine information systems impedes scale-up. This paper evaluates KMC measurement as part of the Every Newborn Birth Indicators Research Tracking in Hospitals (EN-BIRTH) study.
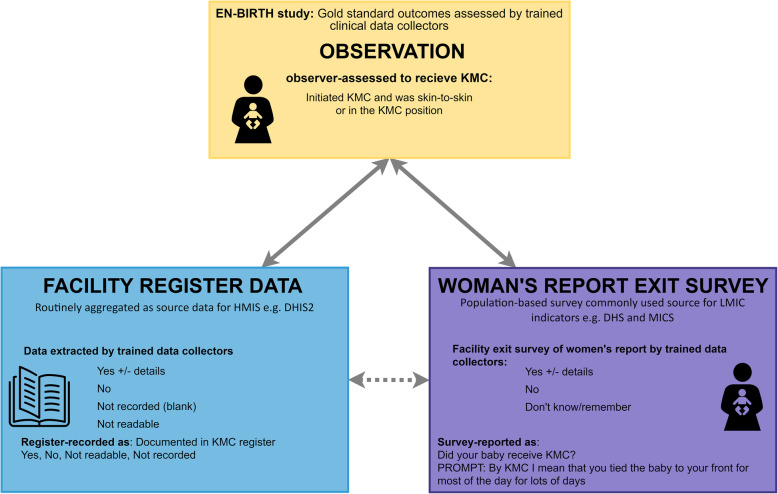
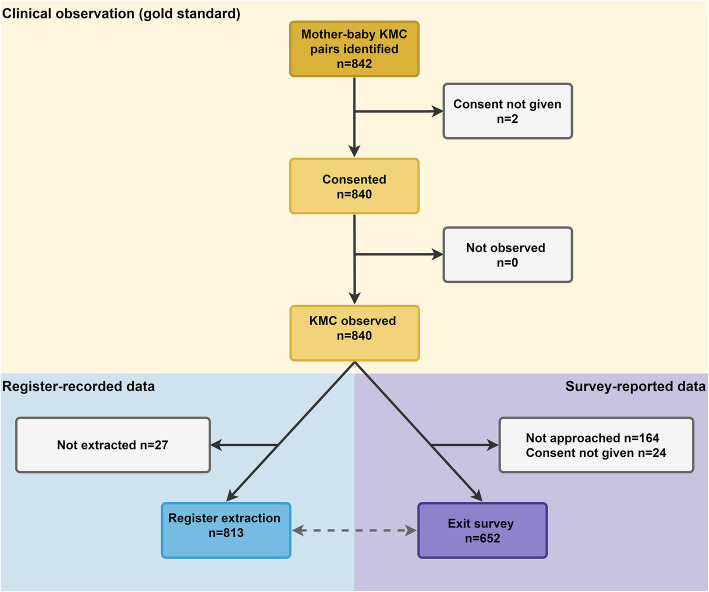
Methods: The EN-BIRTH observational mixed-methods study was conducted in five hospitals in Bangladesh, Nepal and Tanzania from 2017 to 2018. Clinical observers collected time-stamped data as gold standard for mother-baby pairs in KMC wards/corners. To assess accuracy, we compared routine register-recorded and women's exit survey-reported coverage to observed data, using different recommended denominator options (≤2000 g and ≤ 2499 g). We analysed gaps in quality of provision and experience of KMC. In the Tanzanian hospitals, we assessed daily skin-to-skin duration/dose and feeding frequency. Qualitative data were collected from health workers and data collectors regarding barriers and enablers to routine register design, filling and use.
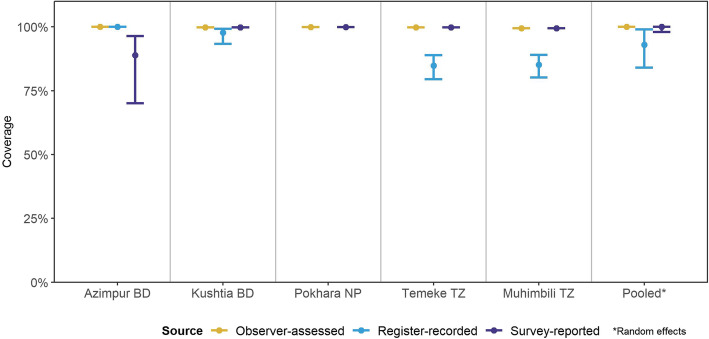
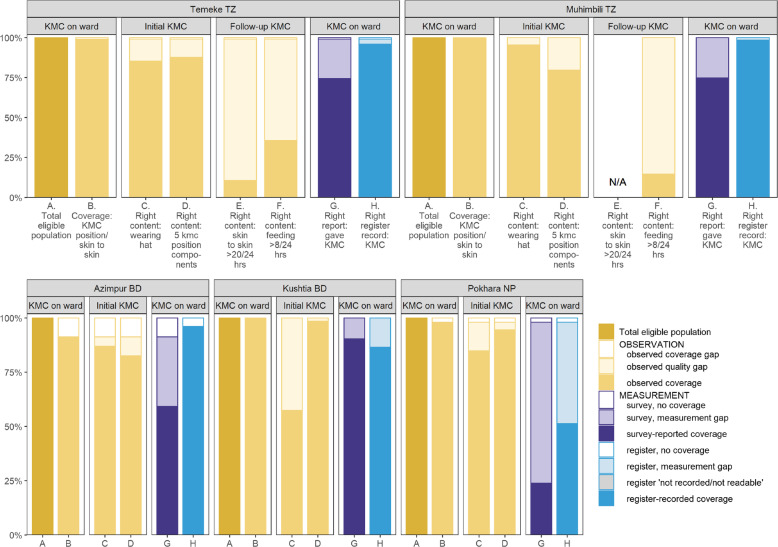
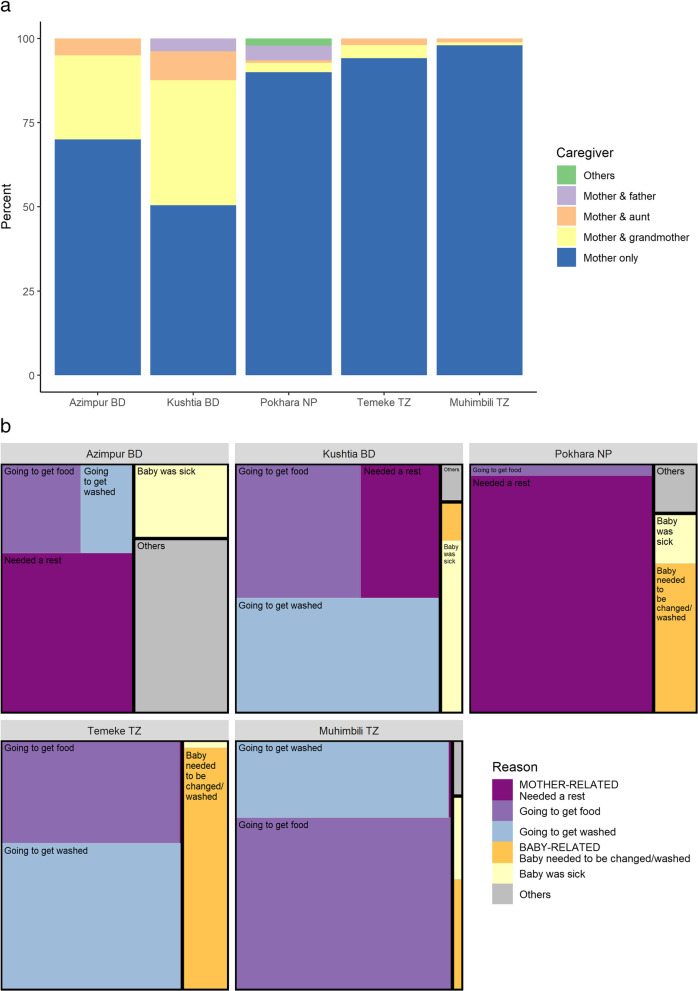
Results: Among 840 mother-baby pairs, compared to observed 100% coverage, both exit-survey reported (99.9%) and register-recorded coverage (92.9%) were highly valid measures with high sensitivity. KMC specific registers outperformed general registers. Enablers to register recording included perceptions of data usefulness, while barriers included duplication of data elements and overburdened health workers. Gaps in KMC quality were identified for position components including wearing a hat. In Temeke Tanzania, 10.6% of babies received daily KMC skin-to-skin duration/dose of ≥20 h and a further 75.3% received 12-19 h. Regular feeding ≥8 times/day was observed for 36.5% babies in Temeke Tanzania and 14.6% in Muhimbili Tanzania. Cup-feeding was the predominant assisted feeding method. Family support during admission was variable, grandmothers co-provided KMC more often in Bangladesh. No facility arrangements for other family members were reported by 45% of women at exit survey.
Conclusions: Routine hospital KMC register data have potential to track coverage from hospital KMC wards/corners. Women accurately reported KMC at exit survey and evaluation for population-based surveys could be considered. Measurement of content, quality and experience of KMC need consensus on definitions. Prioritising further KMC measurement research is important so that high quality data can be used to accelerate scale-up of high impact care for the most vulnerable.
Keywords: Birth; Coverage; Health management systems; Hospital records; Kangaroo mother care; Maternal; Newborn; Preterm; Survey; Validity.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–2172. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
-
- Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of under-5 mortality in 2000-15: an updated systematic analysis with implications for the sustainable development goals. Lancet. 2016;388(10063):3027–3035. doi: 10.1016/S0140-6736(16)31593-8. - DOI - PMC - PubMed
-
- Moxon SG, Lawn JE, Dickson KE, Simen-Kapeu A, Gupta G, Deorari A, Singhal N, New K, Kenner C, Bhutani V, et al. Inpatient care of small and sick newborns: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015;15(Suppl 2):S7. doi: 10.1186/1471-2393-15-S2-S7. - DOI - PMC - PubMed
-
- World Health Organization . WHO recommendations on interventions to improve preterm birth outcomes. 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
