

Development of a novel global rating scale for objective structured assessment of technical skills in an emergency medical simulation training
- PMID: 33766007
- PMCID: PMC7995755
- DOI: 10.1186/s12909-021-02580-4
Development of a novel global rating scale for objective structured assessment of technical skills in an emergency medical simulation training
Abstract
Background: Medical simulation trainings lead to an improvement in patient care by increasing technical and non-technical skills, procedural confidence and medical knowledge. For structured simulation-based trainings, objective assessment tools are needed to evaluate the performance during simulation and the learning progress. In surgical education, objective structured assessment of technical skills (OSATS) are widely used and validated. However, in emergency medicine and anesthesia there is a lack of validated assessment tools for technical skills. Thus, the aim of the present study was to develop and validate a novel Global Rating Scale (GRS) for emergency medical simulation trainings.
Methods: Following the development of the GRS, 12 teams of different experience in emergency medicine (4th year medical students, paramedics, emergency physicians) were involved in a pre-hospital emergency medicine simulation scenario and assessed by four independent raters. Subsequently, interrater reliability and construct validity of the GRS were analyzed. Moreover, the results of the GRS were cross-checked with a task specific check list. Data are presented as median (minimum; maximum).
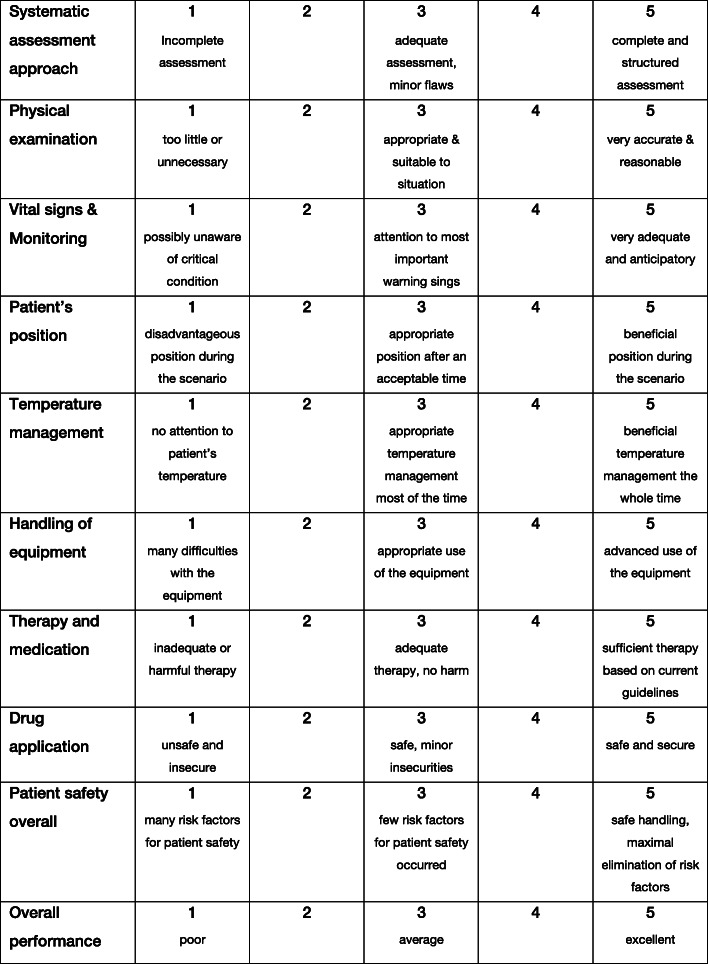
Results: The GRS consists of ten items each scored on a 5-point Likert scale yielding a maximum of 50 points. The median score achieved by novice teams was 22.75 points (17;30), while experts scored 39.00 points (32;47). The GRS overall scores significantly discriminated between student-guided teams and expert teams of emergency physicians (p = 0.005). Interrater reliability for the GRS was high with a Kendall's coefficient of concordance W ranging from 0.64 to 0.90 in 9 of 10 items and 0.88 in the overall score.
Conclusion: The GRS represents a promising novel tool to objectively assess technical skills in simulation training with high construct validity and interrater reliability in this pilot study.
Keywords: Emergency medicine; Global rating scale; Objective structured assessment; Simulation; Technical skills.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Drews FA, Bakdash JZ. Simulation training in health care. Rev Hum Factor Ergonomics. 2013;8(1):191–234. doi: 10.1177/1557234X13492977. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
