

Pharmacy stakeholder reports on ethical and logistical considerations in anti-opioid vaccine development
- PMID: 33766021
- PMCID: PMC7992836
- DOI: 10.1186/s12910-021-00599-2
Pharmacy stakeholder reports on ethical and logistical considerations in anti-opioid vaccine development
Abstract
Background: As opioid use disorder (OUD) incidence and its associated deaths continue to persist at elevated rates, the development of novel treatment modalities is warranted. Recent strides in this therapeutic area include novel anti-opioid vaccine approaches. This work compares logistical and ethical considerations surrounding currently available interventions for opioid use disorder with an anti-opioid vaccine approach.
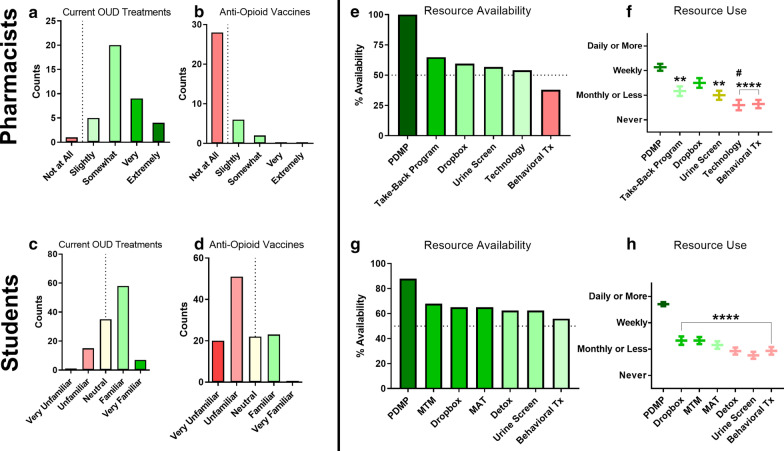
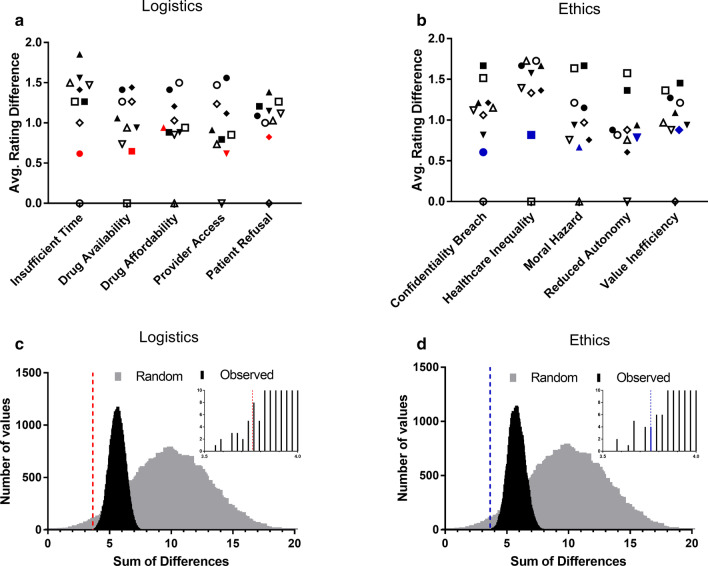
Methods: The opinions of student pharmacists and practicing pharmacists assessing knowledge, perceptions, and attitudes toward current and future OUD management strategies were characterized using a staged, multi-modal research approach incorporating a focus group, pilot survey development and refinement, and final survey deployment. Survey responses were assessed using one- and two-way parametric and non-parametric analyses where appropriate, and multi-dimensional matrix profiles were compared using z-tests following an exhaustive combinatorial sum of differences calculation between items within each compared matrix.
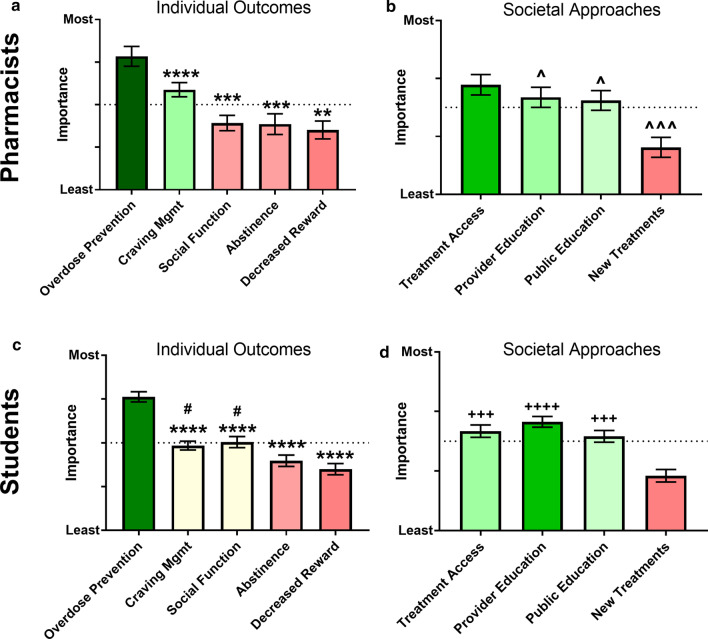
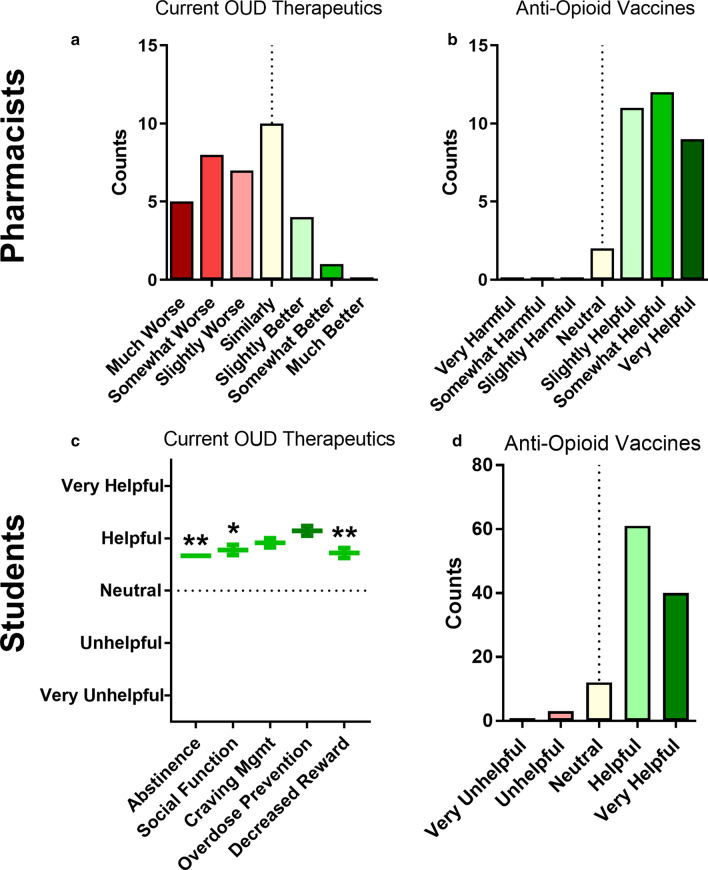
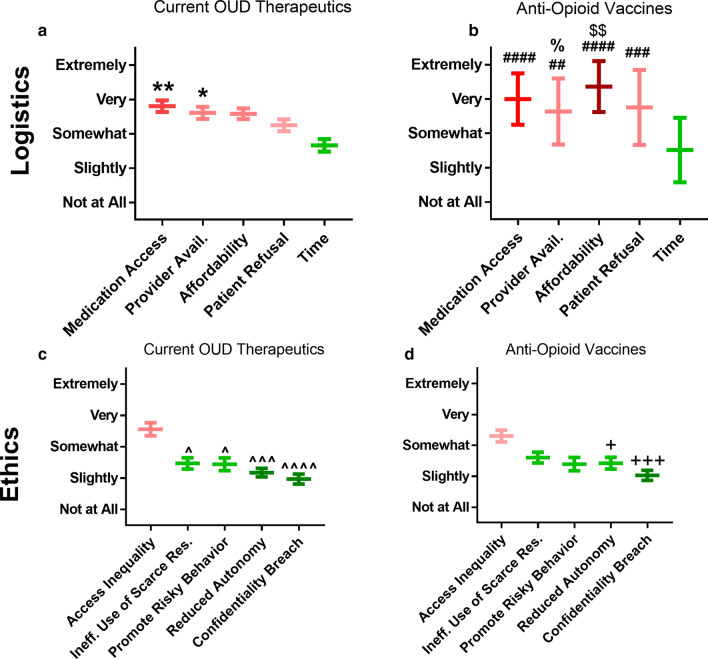
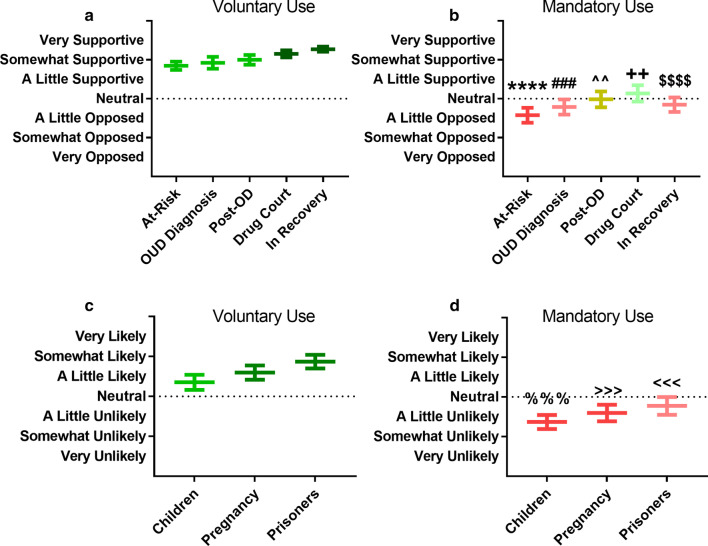
Results: Focus group content analysis revealed a high level of agreeableness among participants regarding anti-opioid vaccine technology and a sense of shared ownership regarding solutions to the opioid epidemic at large. Pilot survey results demonstrated subject ability to consider both pragmatic and ethical considerations related to current therapeutics and novel interventions in a single instrument, with high endurance amongst engaged subjects. Access inequality was the most concerning ethical consideration identified for anti-opioid vaccines. Support for anti-opioid vaccine implementation across various clinical scenarios was strongest for voluntary use amongst individuals in recovery, and lowest for mandatory use in at-risk individuals.
Conclusions: Ethical and logistical concerns surrounding anti-opioid vaccines were largely similar to those for current OUD therapeutics overall. Anti-opioid vaccines were endorsed as helpful potential additions to current OUD therapeutic approaches, particularly for voluntary use in the later stages of clinical progression.
Keywords: Drug development; Ethics; Logistics; Opioid; Stakeholder; Vaccine.
Conflict of interest statement
All authors have no competing interests to disclose.
Figures


Similar articles
-
Evaluating comparative effectiveness of psychosocial interventions adjunctive to opioid agonist therapy for opioid use disorder: A systematic review with network meta-analyses.PLoS One. 2020 Dec 28;15(12):e0244401. doi: 10.1371/journal.pone.0244401. eCollection 2020. PLoS One. 2020. PMID: 33370393 Free PMC article.
-
Supervised dosing with a long-acting opioid medication in the management of opioid dependence.Cochrane Database Syst Rev. 2017 Apr 27;4(4):CD011983. doi: 10.1002/14651858.CD011983.pub2. Cochrane Database Syst Rev. 2017. PMID: 28447766 Free PMC article.
-
Effectiveness of methadone versus buprenorphine in the treatment of opioid use disorder: secondary analyses of prospective cohort study data.BMJ Open. 2025 Jun 17;15(6):e095645. doi: 10.1136/bmjopen-2024-095645. BMJ Open. 2025. PMID: 40527567 Free PMC article.
-
How Is Preoperative Opioid Use Associated With Readmissions and Outcomes in Lower Extremity Trauma?Clin Orthop Relat Res. 2025 May 1;483(5):918-927. doi: 10.1097/CORR.0000000000003346. Epub 2024 Dec 20. Clin Orthop Relat Res. 2025. PMID: 39787379
-
Psychosocial interventions for cannabis use disorder.Cochrane Database Syst Rev. 2016 May 5;2016(5):CD005336. doi: 10.1002/14651858.CD005336.pub4. Cochrane Database Syst Rev. 2016. PMID: 27149547 Free PMC article.
Cited by
-
The Role of the Pharmacist in Combating the Opioid Crisis: An Update.Subst Abuse Rehabil. 2022 Dec 28;13:127-138. doi: 10.2147/SAR.S351096. eCollection 2022. Subst Abuse Rehabil. 2022. PMID: 36597518 Free PMC article. Review.
-
Acceptability of a Fentanyl Vaccine to Prevent Opioid Overdose and Need for Personalized Decision-Making.Clin Infect Dis. 2022 Aug 15;75(Suppl 1):S98-S109. doi: 10.1093/cid/ciac344. Clin Infect Dis. 2022. PMID: 35579508 Free PMC article.
-
The development of opioid vaccines as a novel strategy for the treatment of opioid use disorder and overdose prevention.Int J Neuropsychopharmacol. 2025 Feb 4;28(2):pyaf005. doi: 10.1093/ijnp/pyaf005. Int J Neuropsychopharmacol. 2025. PMID: 39831679 Free PMC article. Review.
References
-
- Petruzzelli M. About the National Council SAMHSA releases national survey on drug use and Health. https://www.thenationalcouncil.org/capitol-connector/2018/09/samhsa-rele....
-
- DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, Ellingrod VL, Haines ST, Nolin TD. Pharmacotherapy: a pathophysiologic approach. New York: McGraw-Hill Education; 2017.
-
- DHHS. Opioid overdoses accounted for more than 42, 000 deaths in 2016, more than any previous year on record. An estimated 40% of opioid overdose deaths involved a prescription opioid. https://www.hhs.gov/opioids/about-the-epidemic/index.html. Accessed November 2019. No Title.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
