

High IRF8 expression correlates with CD8 T cell infiltration and is a predictive biomarker of therapy response in ER-negative breast cancer
- PMID: 33766090
- PMCID: PMC7992828
- DOI: 10.1186/s13058-021-01418-7
High IRF8 expression correlates with CD8 T cell infiltration and is a predictive biomarker of therapy response in ER-negative breast cancer
Erratum in
-
Correction to: High IRF8 expression correlates with CD8 T cell infiltration and is a predictive biomarker of therapy response in ER-negative breast cancer.Breast Cancer Res. 2021 Apr 22;23(1):48. doi: 10.1186/s13058-021-01427-6. Breast Cancer Res. 2021. PMID: 33888121 Free PMC article. No abstract available.
Abstract
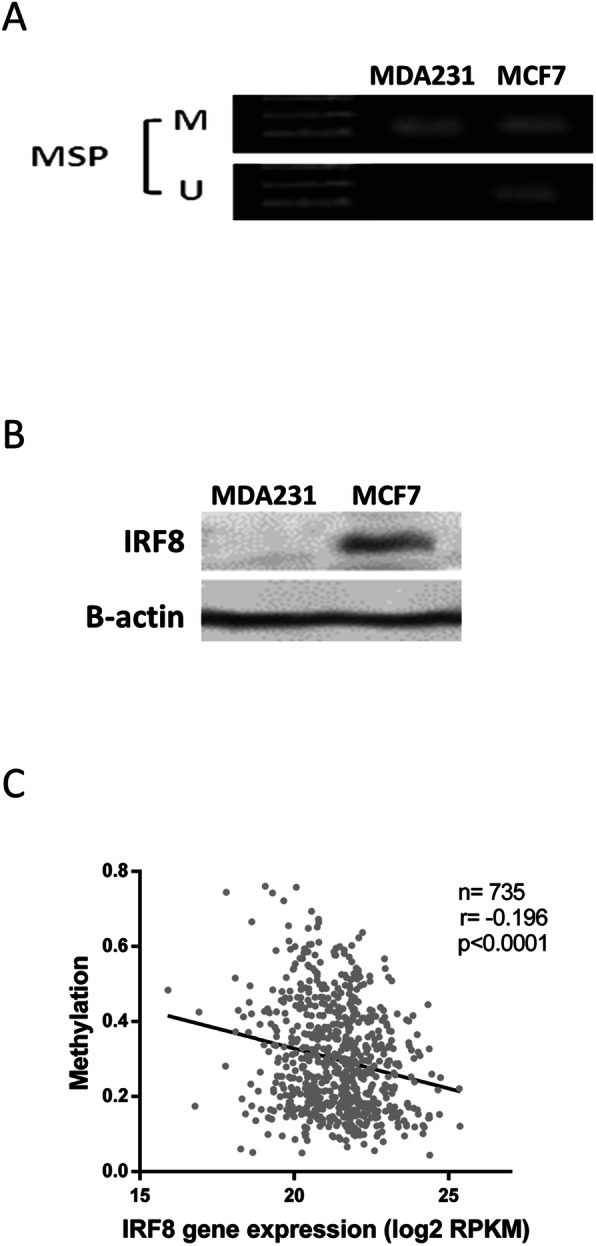
Background: Characterization of breast cancer (BC) through the determination of conventional markers such as ER, PR, HER2, and Ki67 has been useful as a predictive and therapeutic tool. Also, assessment of tumor-infiltrating lymphocytes has been proposed as an important prognostic aspect to be considered in certain BC subtypes. However, there is still a need to identify additional biomarkers that could add precision in distinguishing therapeutic response of individual patients. To this end, we focused in the expression of interferon regulatory factor 8 (IRF8) in BC cells. IRF8 is a transcription factor which plays a well-determined role in myeloid cells and that seems to have multiple antitumoral roles: it has tumor suppressor functions; it acts downstream IFN/STAT1, required for the success of some therapeutic regimes, and its expression in neoplastic cells seems to depend on a cross talk between the immune contexture and the tumor cells. The goal of the present study was to examine the relationship between IRF8 with the therapeutic response and the immune contexture in BC, since its clinical significance in this type of cancer has not been thoroughly addressed.
Methods: We identified the relationship between IRF8 expression and the clinical outcome of BC patients and validated IRF8 as predictive biomarker by using public databases and then performed in silico analysis. To correlate the expression of IRF8 with the immune infiltrate in BC samples, we performed quantitative multiplex immunohistochemistry.
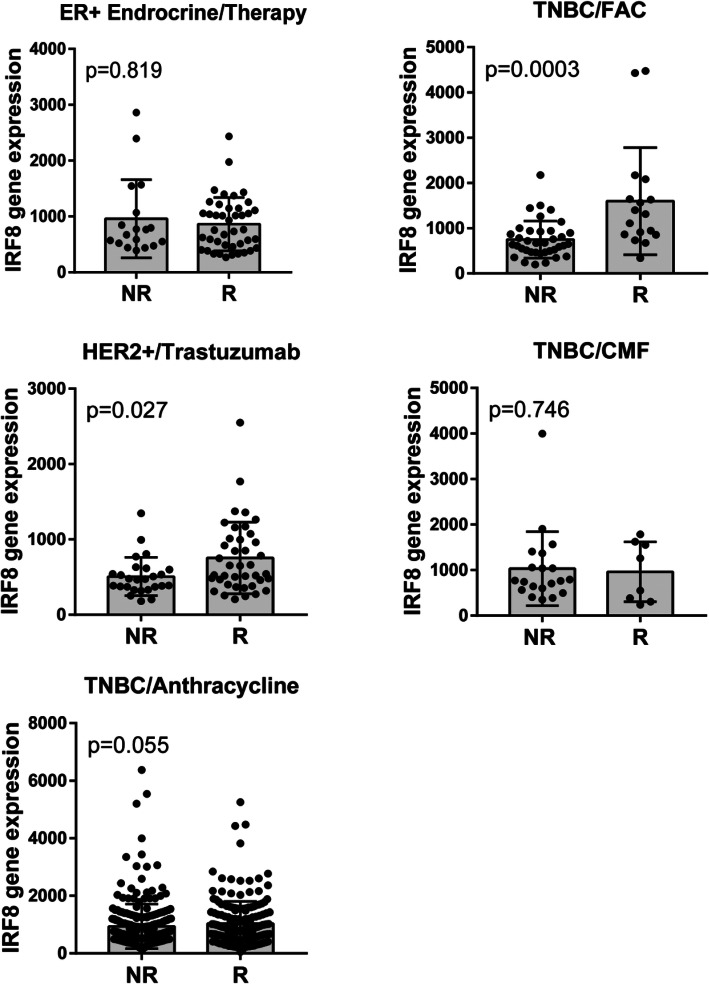
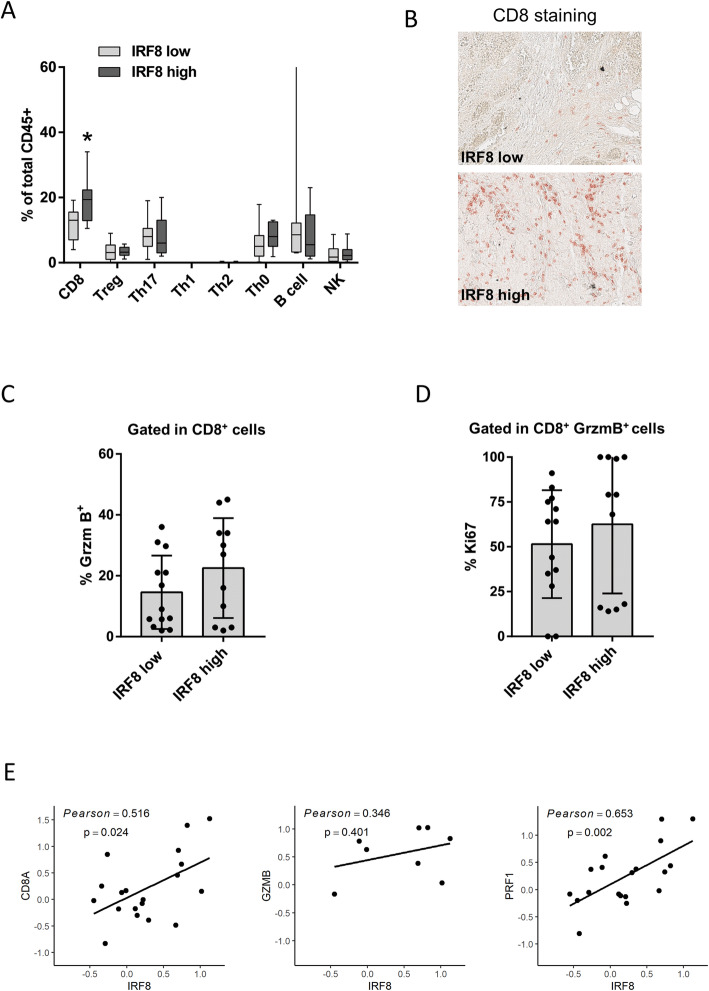
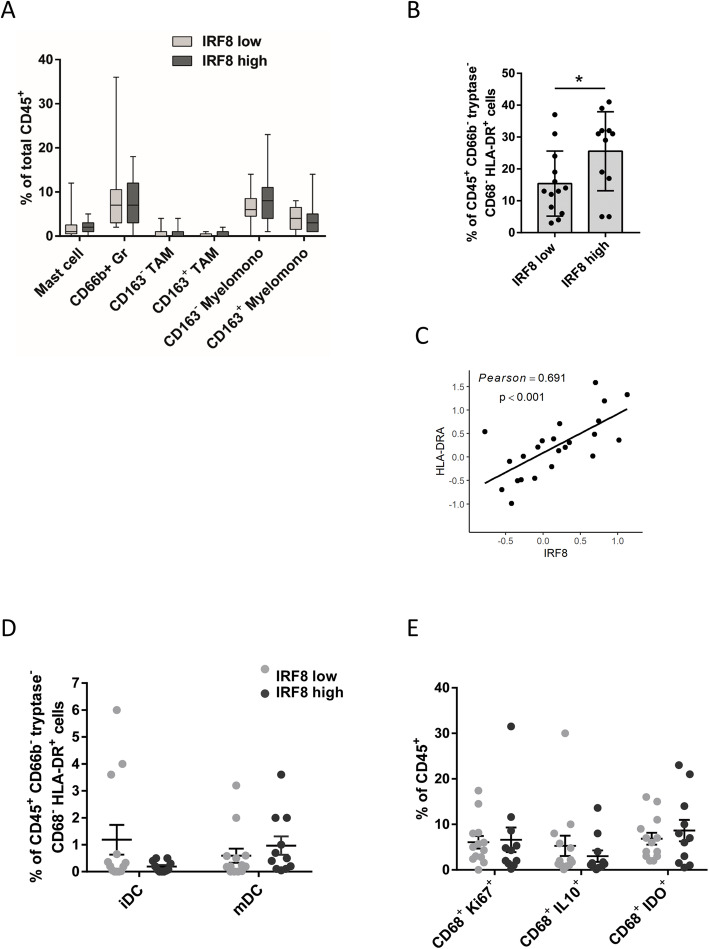
Results: IRF8 expression can precisely predict the complete pathological response to monoclonal antibody therapy or to select combinations of chemotherapy such as FAC (fluorouracil, adriamycin, and cytoxan) in ER-negative BC subtypes. Analysis of immune cell infiltration indicates there is a strong correlation between activated and effector CD8+ T cell infiltration and tumoral IRF8 expression.
Conclusions: We propose IRF8 expression as a potent biomarker not only for prognosis, but also for predicting therapy response in ER-negative BC phenotypes. Its expression in neoplastic cells also correlates with CD8+ T cell activation and infiltration. Therefore, our results justify new efforts towards understanding mechanisms regulating IRF8 expression and how they can be therapeutically manipulated.
Keywords: Breast cancer; DNA methylation; IRF8; Predictive marker; Tumor-infiltrate.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Holtschke T, Löhler J, Kanno Y, Fehr T, Giese N, Rosenbauer F, Lou J, Knobeloch KP, Gabriele L, Waring JF, Bachmann MF, Zinkernagel RM, Morse HC, III, Ozato K, Horak I. Immunodeficiency and chronic myelogenous leukemia-like syndrome in mice with a targeted mutation of the ICSBP gene. Cell. 1996;87(2):307–317. doi: 10.1016/S0092-8674(00)81348-3. - DOI - PubMed
-
- Kim SH, Burton J, Yu CR, Sun L, He C, Wang H, Morse HC, 3rd, Egwuagu CE. Dual-function of the IRF8 transcription factor in autoimmune uveitis: loss of IRF8 in T cells exacerbates uveitis while Irf8 deletion in the retina confers protection. J Immunol. 2015;195(4):1480–1488. doi: 10.4049/jimmunol.1500653. - DOI - PMC - PubMed
-
- Bagadia P, Huang X, Liu TT, Durai V, Grajales-Reyes GE, Nitschké M, Modrusan Z, Granja JM, Satpathy AT, Briseño CG, Gargaro M, Iwata A, Kim S, Chang HY, Shaw AS, Murphy TL, Murphy KM. An Nfil3-Zeb2-Id2 pathway imposes Irf8 enhancer switching during cDC1 development. Nat Immunol. 2019;20(9):1174–1185. doi: 10.1038/s41590-019-0449-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
