

Neurolymphomatosis of the median nerve, optic nerve, L4 spinal nerve root and cauda equina in patients with B-cell malignancies: a case series
- PMID: 33766128
- PMCID: PMC7995761
- DOI: 10.1186/s13256-021-02714-8
Neurolymphomatosis of the median nerve, optic nerve, L4 spinal nerve root and cauda equina in patients with B-cell malignancies: a case series
Abstract
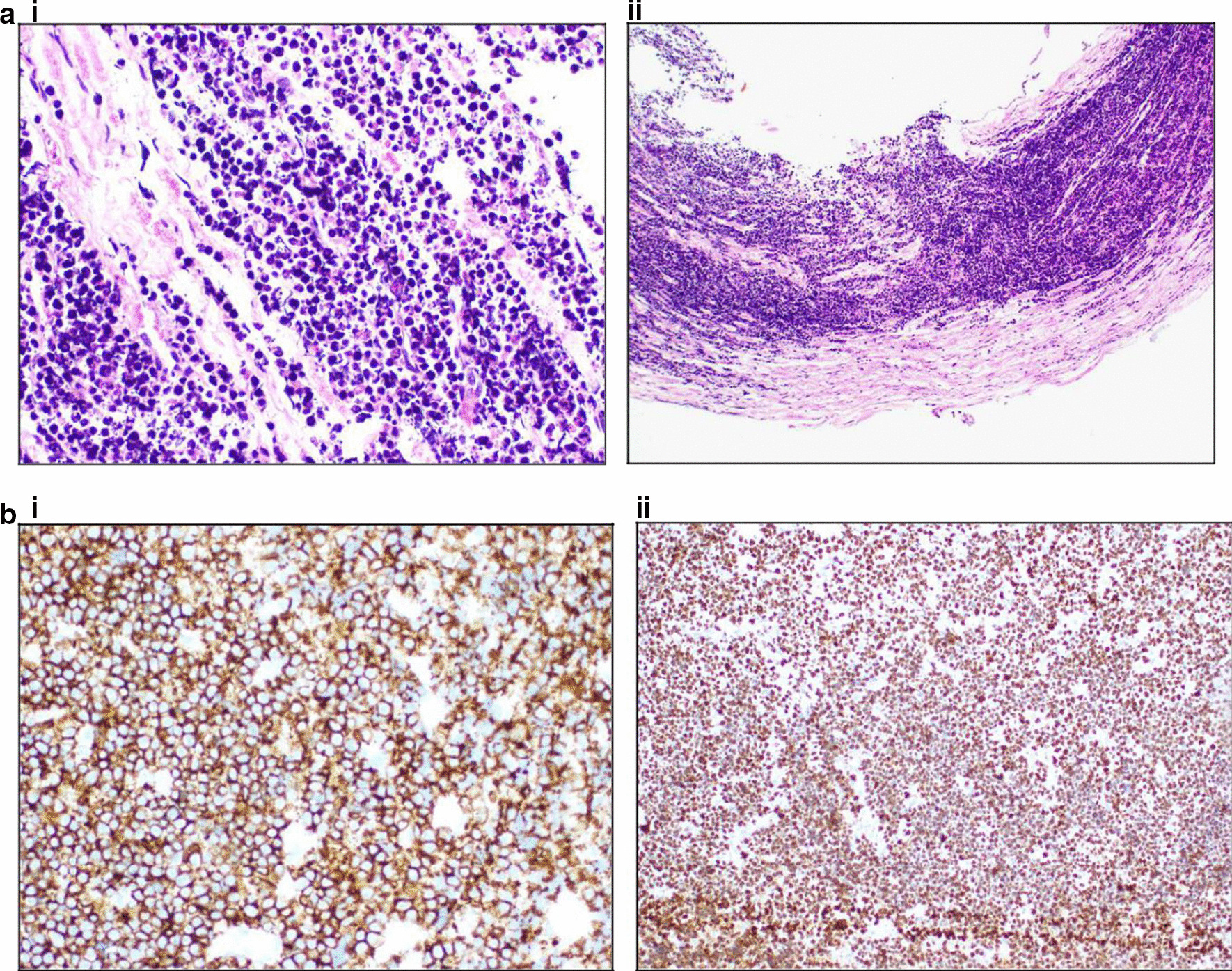
Background: Neurolymphomatosis is rare. Neoplastic lymphocytes are seen to invade nerves (cranial or peripheral), nerve roots or other related structures in patients with hematological malignancy. It is a separate entity from central nervous system lymphoma. Neurolymphomatosis has most commonly been described in association with B-cell non-Hodgkin lymphoma. Neurolymphomatosis in the context of Burkitt lymphoma and the post-renal transplant setting has not been described before.
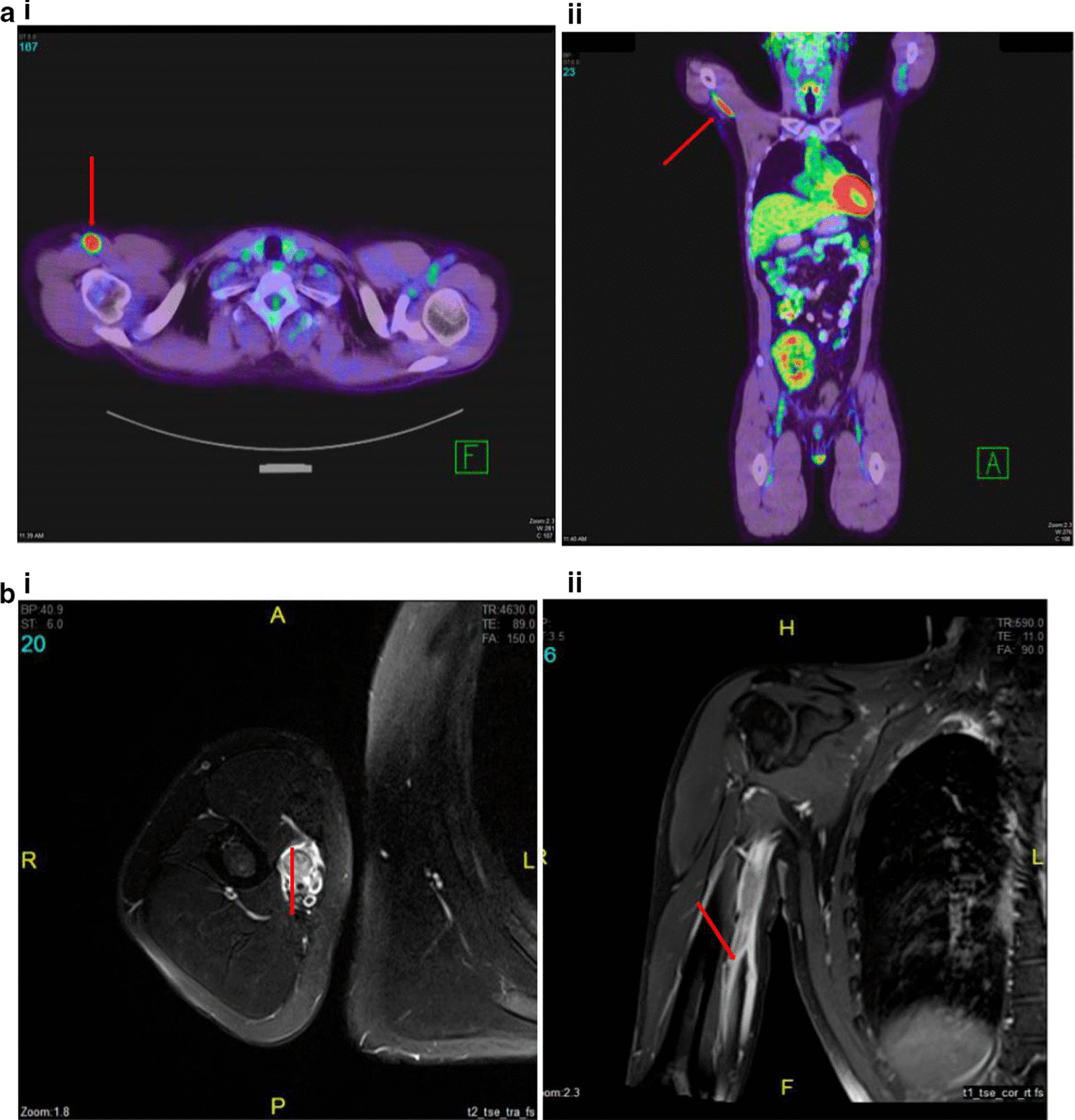
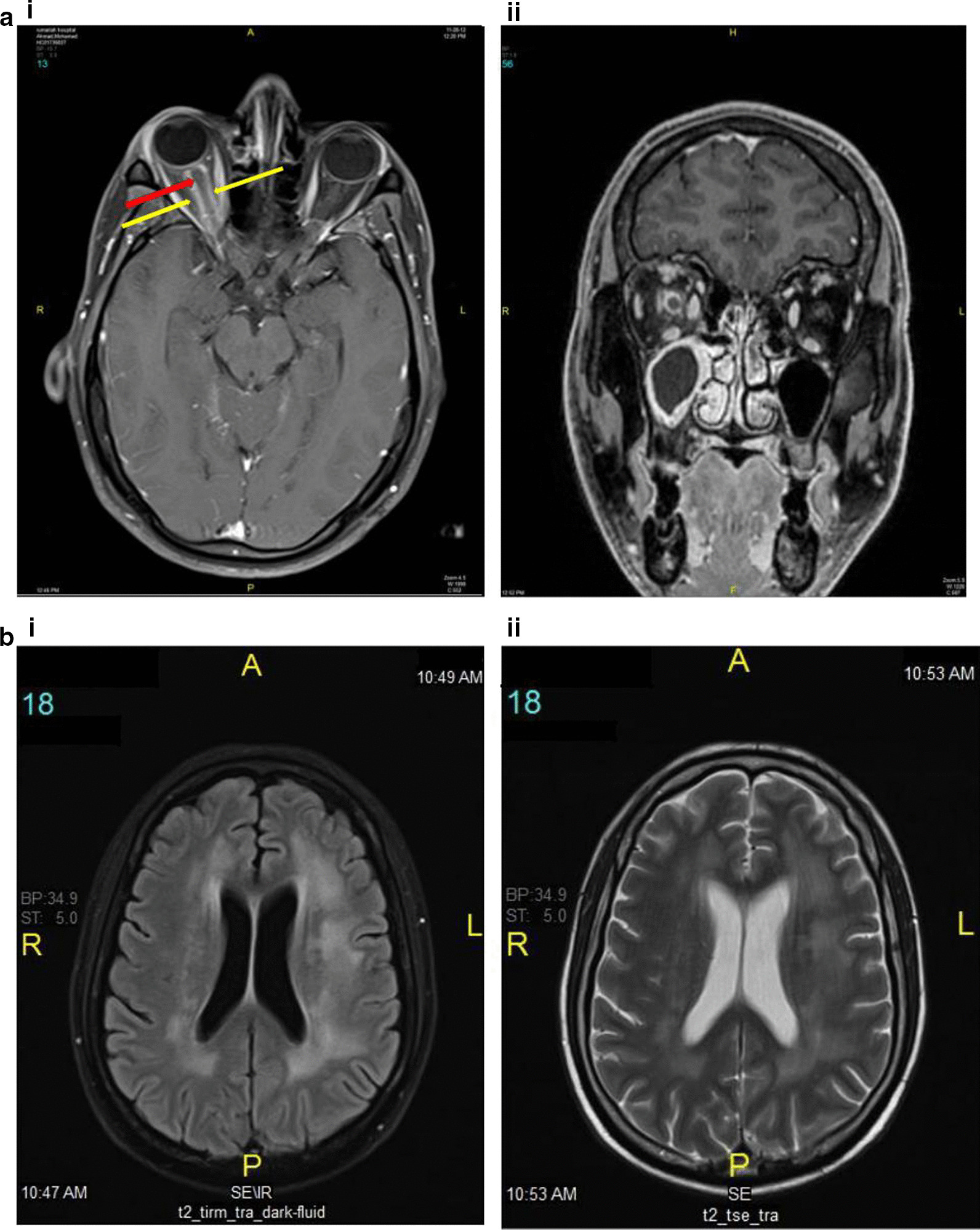
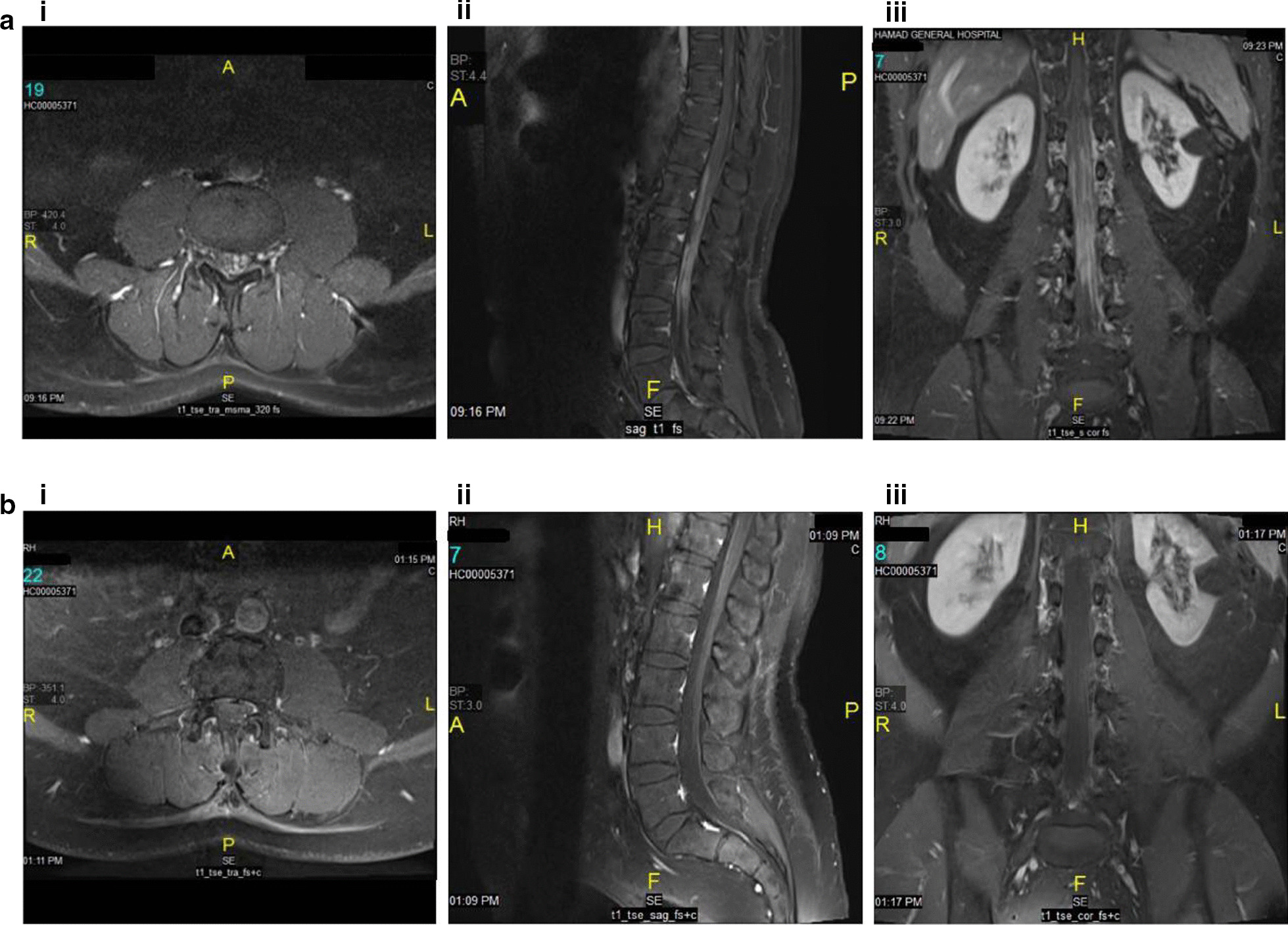
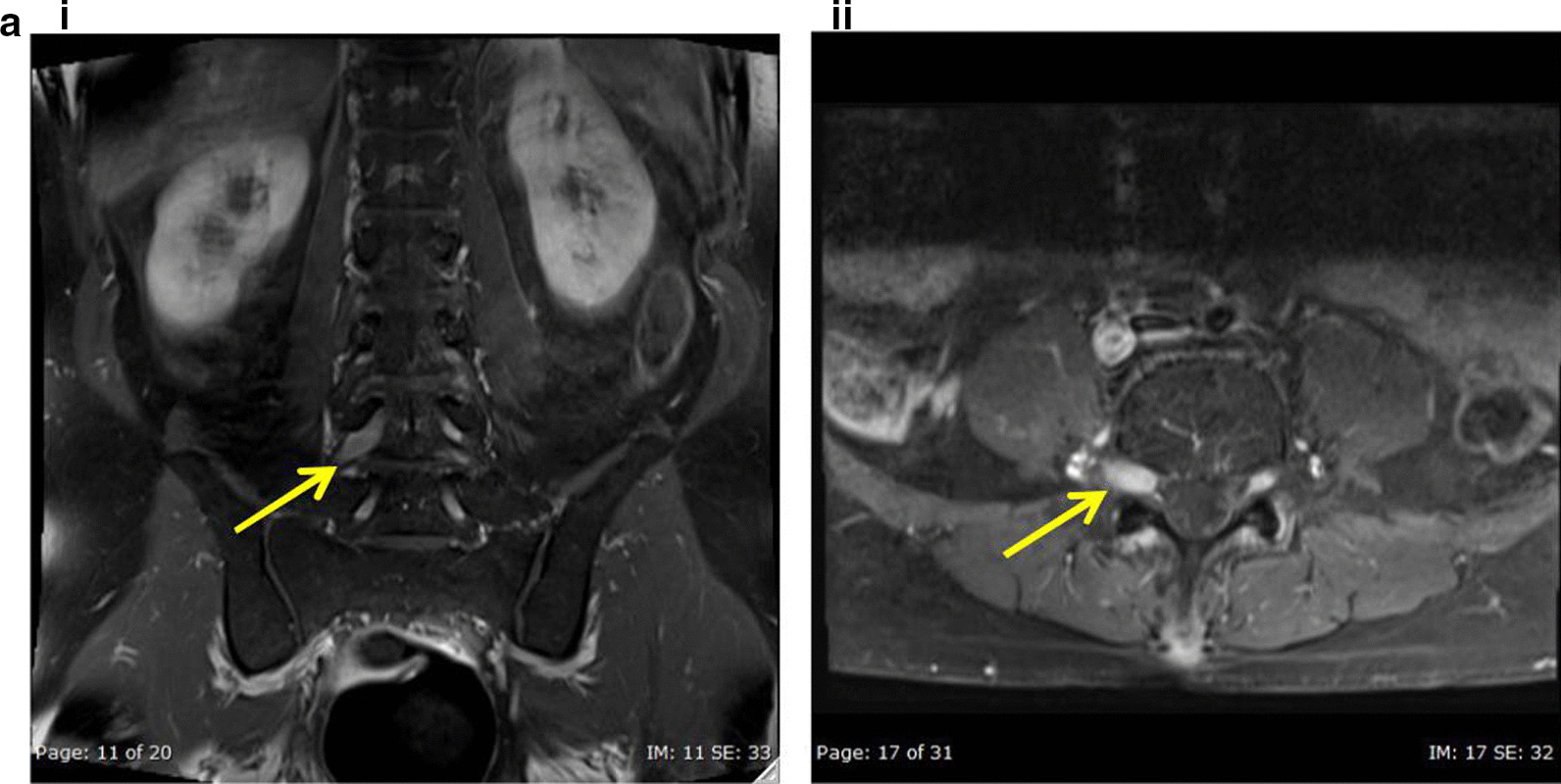
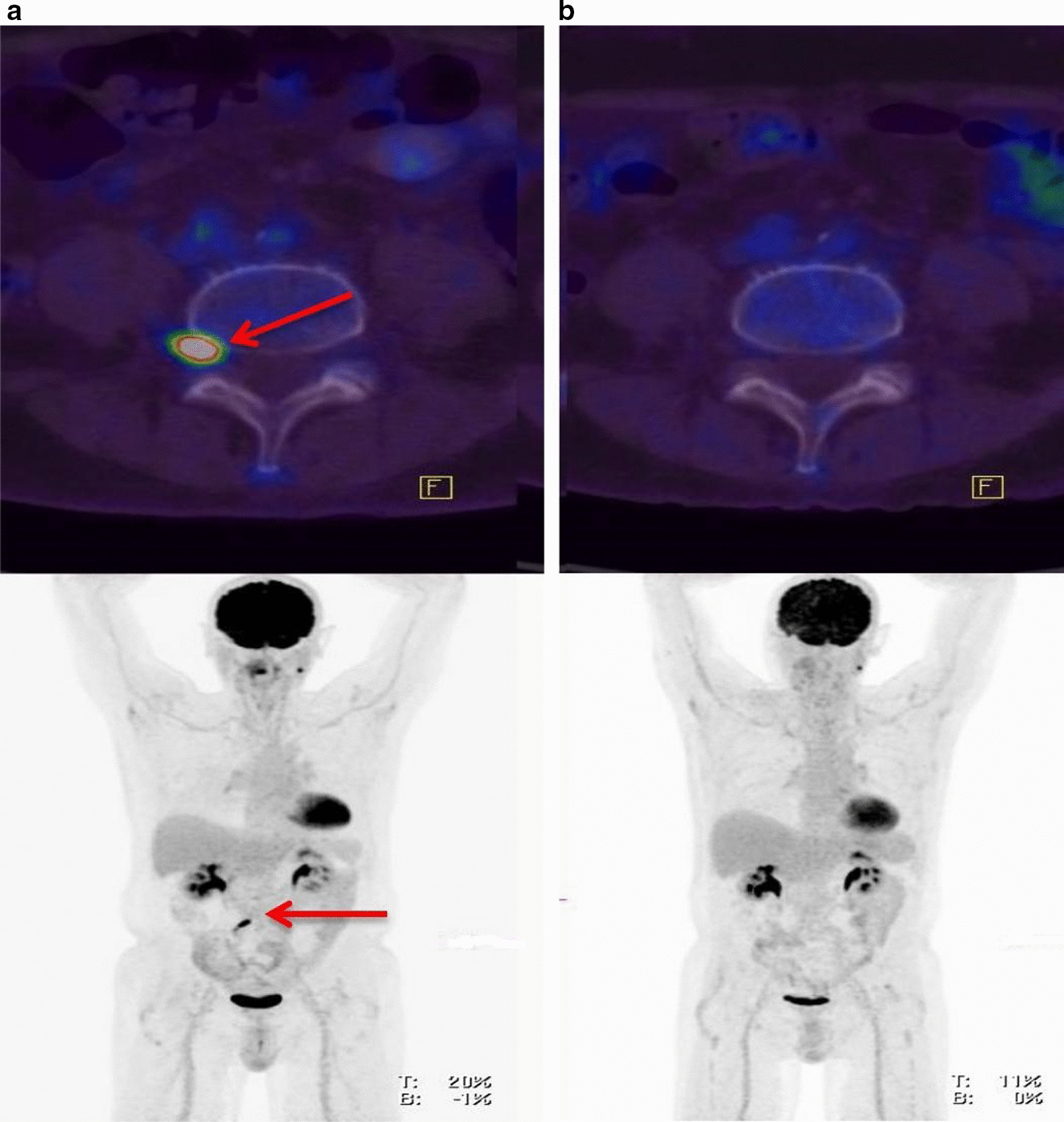
Case reports: We report for the first time in the Arabian Gulf countries and nearby Arab states four cases of neurolymphomatosis (one Asian, and the other 3 are from Arabic nationals) occurring between 2012 and 2017 involving the median nerve, optic nerve, nerve root and cauda equina in patients with Burkitt lymphoma, Philadelphia chromosome-positive B-cell acute lymphoblastic leukemia and diffuse large B-cell lymphoma.
Conclusions: Neurolymphomatosis is rare and can be difficult to diagnose by biopsy but reliably confirmed by a combined imaging approach. Prior treatment with high-dose dexamethasone might suppress 18F-fluorodeoxyglucose (FDG) activity and decrease the sensitivity of positron emission tomography/computed tomography (PET/CT). The prognosis is generally poor but using high-dose methotrexate as well as high-dose chemotherapy and autologous stem cell transplantation may be an effective way to treat neurolymphomatosis.
Keywords: B cell-acute lymphoblastic leukemia (b-ALL); Burkitt lymphoma; Cauda equina syndrome; Diffuse large B-cell lymphoma; L4 spinal nerve root; Median nerve palsy; Neurolymphomatosis; Optic nerve lesion; Post-transplant lymphoproliferative disorder (PTLD); Renal transplant.
Conflict of interest statement
None of the authors have any competing interests relating to this article.
Figures
Similar articles
-
Primary cauda equina lymphoma confirmed by autopsy: A case report.Neuropathology. 2024 Apr;44(2):147-153. doi: 10.1111/neup.12941. Epub 2023 Aug 28. Neuropathology. 2024. PMID: 37640533 Review.
-
Neurolymphomatosis in the Cauda Equina Diagnosed by an Open Biopsy.Intern Med. 2018 Dec 1;57(23):3463-3465. doi: 10.2169/internalmedicine.1049-18. Epub 2018 Aug 10. Intern Med. 2018. PMID: 30101916 Free PMC article.
-
Primary Central Nervous System Lymphoma With Diffuse Neurolymphomatosis Involving Multiple Cranial and Spinal Nerve Roots.Clin Nucl Med. 2020 Jun;45(6):e285-e287. doi: 10.1097/RLU.0000000000003018. Clin Nucl Med. 2020. PMID: 32332304
-
Primary Cauda Equina Lymphoma Treated with CNS-Centric Approach: A Case Report and Literature Review.J Blood Med. 2021 Jul 21;12:645-652. doi: 10.2147/JBM.S325264. eCollection 2021. J Blood Med. 2021. PMID: 34321945 Free PMC article.
-
The role of 18F-FDG PET/CT in Neurolymphomatosis: A Comprehensive Imaging Approach.J Pak Med Assoc. 2024 Apr;74(4):822-824. doi: 10.47391/JPMA.24-30. J Pak Med Assoc. 2024. PMID: 38751291 Review.
Cited by
-
The Surgical Histopathology of the Filum Terminale: Findings from a Large Series of Patients with Tethered Cord Syndrome.J Clin Med. 2023 Dec 19;13(1):6. doi: 10.3390/jcm13010006. J Clin Med. 2023. PMID: 38202013 Free PMC article.
-
Metachronous spinal cord involvement B cell and subcutaneous tissue involvement NK/T cell lymphoid proliferations and lymphomas arising in post-transplantation mimicking general NK/T cell lymphoma: a case report and review of the literature.Front Immunol. 2024 Oct 14;15:1467506. doi: 10.3389/fimmu.2024.1467506. eCollection 2024. Front Immunol. 2024. PMID: 39469712 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
