

A non-randomised feasibility study of an intervention to optimise medicines at transitions of care for patients with heart failure
- PMID: 33766141
- PMCID: PMC7995719
- DOI: 10.1186/s40814-021-00819-x
A non-randomised feasibility study of an intervention to optimise medicines at transitions of care for patients with heart failure
Abstract
Background: Heart failure affects 26 million people globally, and the optimal management of medicines is crucial for patients, particularly when their care is transferred between hospital and the community. Optimising clinical outcomes requires well-calibrated cross-organisational processes with staff and patients responding and adapting to medicines changes. The aim of this study was to assess the feasibility of implementing a complex intervention (the Medicines at Transitions Intervention; MaTI) co-designed by patients and healthcare staff. The purpose of the intervention was to optimise medicines management across the gaps between secondary and primary care when hospitals handover care. The study objectives were to (1) assess feasibility through meeting specified progression criteria to proceed to the trial, (2) assess if the intervention was acceptable to staff and patients, and (3) determine whether amendment or refinement would be needed to enhance the MaTI.
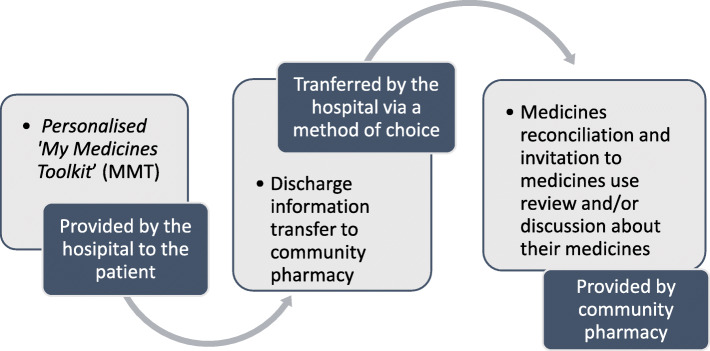
Methods: The feasibility of the MaTI was tested in three healthcare areas in the North of England between July and October 2017. Feasibility was measured and assessed through four agreed progression to trial criteria: (1) patient recruitment, (2) patient receipt of a medicines toolkit, (3) transfer of discharge information to community pharmacy, and (4) offer of a community pharmacy medicines review/discussion or medicines reconciliation. From the cardiology wards at each of the three NHS Acute Trusts (sites), 10 patients (aged ≥ 18 years) were recruited and introduced to the 'My Medicines Toolkit' (MMT). Patients were asked to identify their usual community pharmacy or nominate a pharmacy. Discharge information was transferred to the community pharmacy; pharmacists were asked to reconcile medicines and invited patients for a medicines use review (MUR) or discussion. At 1 month following discharge, all patients were sent three questionnaire sets: quality-of-life, healthcare utilisation, and a patient experience survey. In a purposive sample, 20 patients were invited to participate in a semi-structured interview about their experiences of the MaTI. Staff from hospital and primary care settings involved in patients' care were invited to participate in a semi-structured interview. Patient and staff interviews were analysed using Framework Analysis. Questionnaire completion rates were recorded and data were descriptively analysed.
Results: Thirty-one patients were recruited across three sites. Eighteen staff and 18 patients took part in interviews, and 19 patients returned questionnaire sets. All four progression to trial criteria were met. We identified barriers to patient engagement with the intervention in hospital, which were compounded by patients' focus on returning home. Some patients described not engaging in discussions with staff about medicines and lacking motivation to do so because they were preoccupied with returning home. Some patients were unable or unwilling to attend a community pharmacy in person for a medicines review. Roles and responsibilities for delivering the MaTI were different in the three sites, and staff reported variations in time spent on MaTI activities. Staff reported some work pressures and staff absences that limited the time they could spend talking to patients about their medicines. Clinical teams reported that recording a target dose for heart failure medicines in patient-held documentation was difficult as they did not always know the ideal or tolerable dose. The majority of patients reported receiving the patient-held documentation. More than two-thirds reported being offered a MUR by their community pharmacists.
Conclusions: Delivery of the Medicines at Transitions Intervention (MaTI) was feasible at all three sites, and progression to trial criteria were met. Refinements were found to be necessary to overcome identified barriers and strengthen delivery of all steps of the intervention. Necessary changes to the MaTI were identified along with amendments to the implementation plan for the subsequent trial. Future implementation needs to take into account the complexity of medicines management and adaptation to local context.
Keywords: Cardiology; Care transitions; Clinical trials; Complex intervention; Feasibility studies; Heart failure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Using routine healthcare data to evaluate the impact of the Medicines at Transitions Intervention (MaTI) on clinical outcomes of patients hospitalised with heart failure: protocol for the Improving the Safety and Continuity Of Medicines management at Transitions of care (ISCOMAT) cluster randomised controlled trial with embedded process evaluation, health economics evaluation and internal pilot.BMJ Open. 2022 Apr 29;12(4):e054274. doi: 10.1136/bmjopen-2021-054274. BMJ Open. 2022. PMID: 35487708 Free PMC article.
-
Implementing a Medicines at Transitions Intervention (MaTI) for patients with heart failure: a process evaluation of the Improving the Safety and Continuity Of Medicines management at Transitions of care (ISCOMAT) cluster randomised controlled trial.BMC Health Serv Res. 2024 Oct 9;24(1):1210. doi: 10.1186/s12913-024-11487-x. BMC Health Serv Res. 2024. PMID: 39385160 Free PMC article. Clinical Trial.
-
Experiences of patients with heart failure with medicines at transition intervention: Findings from the process evaluation of the Improving the Safety and Continuity of Medicines management at Transitions of care (ISCOMAT) programme.Health Expect. 2022 Oct;25(5):2503-2514. doi: 10.1111/hex.13570. Epub 2022 Jul 31. Health Expect. 2022. PMID: 35909321 Free PMC article. Clinical Trial.
-
Investigating the organisational factors associated with variation in clinical productivity in community pharmacies: a mixed-methods study.Southampton (UK): NIHR Journals Library; 2017 Oct. Southampton (UK): NIHR Journals Library; 2017 Oct. PMID: 29039899 Free Books & Documents. Review.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Continuous Remote Patient Monitoring in Patients With Heart Failure (Cascade Study): Protocol for a Mixed Methods Feasibility Study.JMIR Res Protoc. 2022 Aug 25;11(8):e36741. doi: 10.2196/36741. JMIR Res Protoc. 2022. PMID: 36006689 Free PMC article.
-
Informational continuity of medication management in transitions of care: Qualitative interviews with stakeholders from the HYPERION-TransCare study.PLoS One. 2024 Apr 4;19(4):e0300047. doi: 10.1371/journal.pone.0300047. eCollection 2024. PLoS One. 2024. PMID: 38573912 Free PMC article.
-
Using routine healthcare data to evaluate the impact of the Medicines at Transitions Intervention (MaTI) on clinical outcomes of patients hospitalised with heart failure: protocol for the Improving the Safety and Continuity Of Medicines management at Transitions of care (ISCOMAT) cluster randomised controlled trial with embedded process evaluation, health economics evaluation and internal pilot.BMJ Open. 2022 Apr 29;12(4):e054274. doi: 10.1136/bmjopen-2021-054274. BMJ Open. 2022. PMID: 35487708 Free PMC article.
-
Using a digital health intervention "INTERCEPT" to improve secondary prevention in coronary heart disease (CHD) patients: protocol for a mixed methods non-randomised feasibility study.HRB Open Res. 2025 Jan 31;6:43. doi: 10.12688/hrbopenres.13781.2. eCollection 2023. HRB Open Res. 2025. PMID: 38414839 Free PMC article.
-
Implementing a Medicines at Transitions Intervention (MaTI) for patients with heart failure: a process evaluation of the Improving the Safety and Continuity Of Medicines management at Transitions of care (ISCOMAT) cluster randomised controlled trial.BMC Health Serv Res. 2024 Oct 9;24(1):1210. doi: 10.1186/s12913-024-11487-x. BMC Health Serv Res. 2024. PMID: 39385160 Free PMC article. Clinical Trial.
References
-
- Ambrosy AP, Fonarow GC, Butler J, Chioncel O, Greene SJ, Vaduganathan M, Nodari S, Lam CSP, Sato N, Shah AN, Gheorghiade M. The global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registries. J Am Coll Cardiol. 2014;63(12):1123–1133. doi: 10.1016/j.jacc.2013.11.053. - DOI - PubMed
-
- Konstam MA, Neaton JD, Dickstein K, Drexler H, Komajda M, Martinez FA, Riegger GAJ, Malbecq W, Smith RD, Guptha S, Poole-Wilson PA. Effects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure (HEAAL study): a randomised, double-blind trial. Lancet. 2009;374(9704):1840–1848. doi: 10.1016/S0140-6736(09)61913-9. - DOI - PubMed
-
- Authors/Task Force Members, McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Böhm M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. Eur J Heart Fail. 2012;14(8):803–69. 10.1093/eurjhf/hfs105. - PubMed
-
- Fylan B, Tranmer M, Armitage G, Blenkinsopp A. Fylan B, Tranmer M, Armitage G, Blenkinsopp A. Cardiology patients’ medicines management networks after hospital discharge: a mixed methods analysis of a complex adaptive system. Res Soc Adm Pharm. 2019;15(5):505-513. doi:10.1016/j.sapharm.2018.06.016 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
